Kubota Akatsuki, Ishiura Hiroyuki, Mitsui Jun, Sakuishi Kaori, Iwata Atsushi, Yamamoto Tomotaka, Nishino Ichizo, Tsuji Shoji, Shimizu Jun
Department of Neurology, The University of Tokyo, Japan.
Department of Neuromuscular Research, National Center of Neurology and Psychiatry, Japan.
Intern Med. 2018 Mar 15;57(6):877-882. doi: 10.2169/internalmedicine.9588-17. Epub 2017 Dec 8.
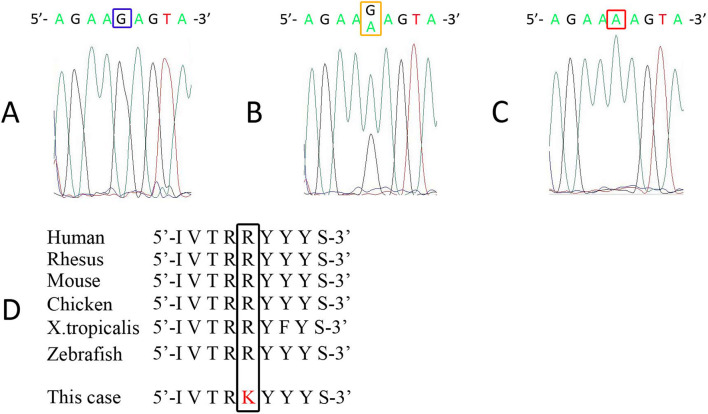
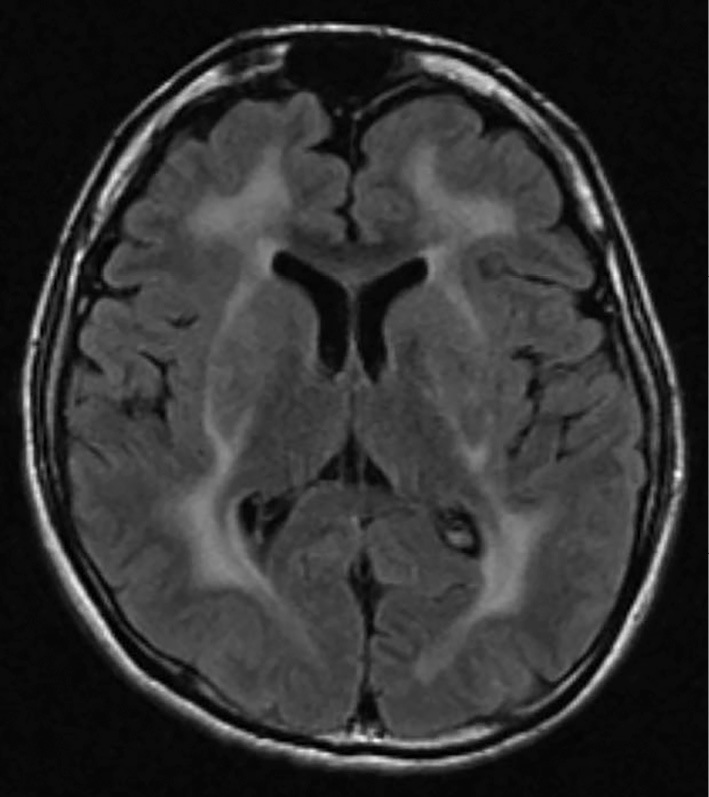
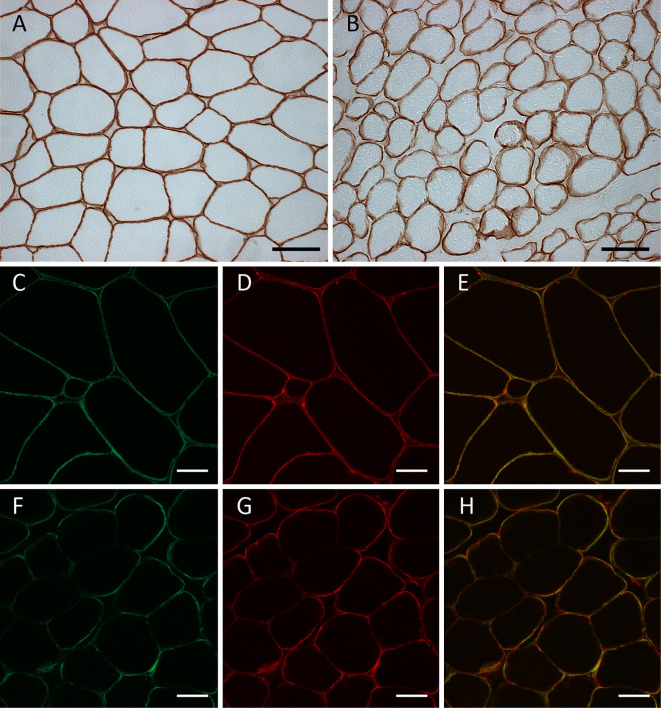
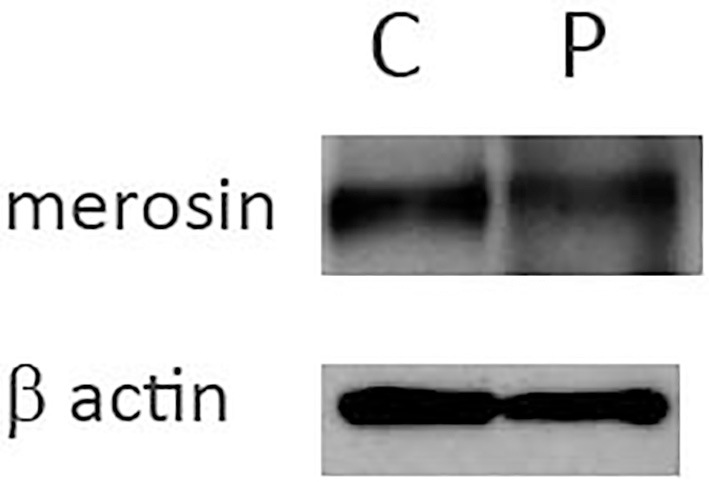
A complete loss of merosin, which is encoded by LAMA2, causes congenital muscular dystrophy with leukoencephalopathy. Partial merosin deficiency can be caused not only by primarily LAMA2 mutations, but also secondarily by dystroglycanopathy. Although it can be molecularly diagnosed based on a genetic analysis, this method is labor-intensive because of its huge genome size. A 26-year-old male patient presented with mild muscular weakness, joint contractures, and epilepsy. Double immunofluorescence staining of a muscle biopsy specimen showed mislocalization of merosin, and a genetic analysis revealed a homozygous c.818G>A (p.Arg273Lys) mutation in LAMA2. Double immunofluorescence staining and whole exome sequencing were useful for the diagnosis of partial merosin deficiency.
由LAMA2编码的merosin完全缺失会导致伴有白质脑病的先天性肌营养不良。部分merosin缺乏不仅可由原发性LAMA2突变引起,也可由继发于糖基化缺陷病引起。虽然可以通过基因分析进行分子诊断,但由于其基因组庞大,这种方法劳动强度大。一名26岁男性患者表现为轻度肌无力、关节挛缩和癫痫。肌肉活检标本的双重免疫荧光染色显示merosin定位错误,基因分析显示LAMA2存在纯合的c.818G>A(p.Arg273Lys)突变。双重免疫荧光染色和全外显子组测序有助于诊断部分merosin缺乏。