Pediatr Infect Dis J. 2018 Apr;37(4):349-355. doi: 10.1097/INF.0000000000001867.
In developing countries, malnutrition remains a common clinical syndrome at antiretroviral treatment (ART) initiation. Physiologic changes because of malnutrition and during nutritional recovery could affect the pharmacokinetics of antiretroviral drugs.
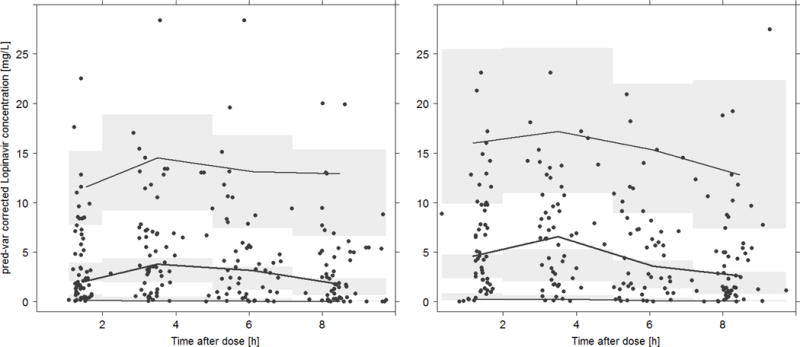
HIV-infected children admitted with severe acute malnutrition were randomized to early or delayed initiation of lopinavir (LPV)/ritonavir, abacavir and lamivudine using World Health Organization weight band dosage charts. LPV concentrations were measured on day 1 and day 14. Thereafter, patients were followed-up to week 48. The population pharmacokinetics of LPV was described using NONMEM v7.3. Covariates were screened to assess their influence on the pharmacokinetics of LPV, and the relationship between pharmacokinetic variability and treatment outcomes were assessed.
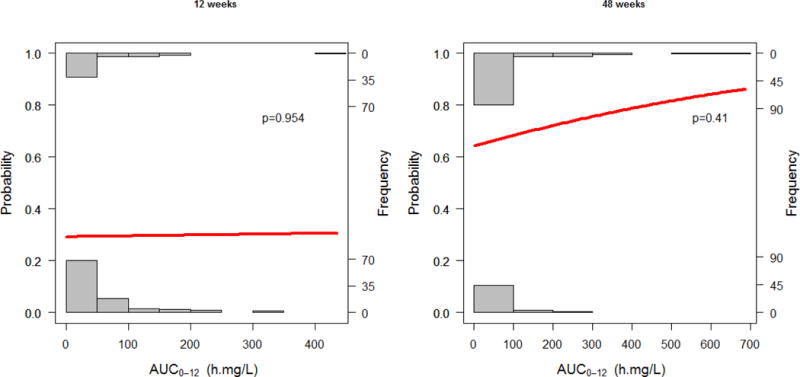
Five hundred and two LPV concentrations were collected from 62 pediatric patients 0.1-3.9 years of age (median: 0.9 years). Rifampin-based antituberculosis treatment and "super-boosted" LPV/ritonavir were prescribed in 20 patients. LPV disposition was well described by a one-compartment model with first-order elimination. Neither randomization to early or delayed ART, tuberculosis comedications nor anthropometrical measurements explained the pharmcokinetic variability. Allometrically scaled fat-free mass influenced apparent clearance (CL/F) and volume of distribution (Vd/F). Pharmacokinetic exposure did not correlate with virologic outcomes or death at 12 or 48 weeks.
LPV pharmacokinetics was influenced by fat-free mass and not by timing of ART initiation or tuberculosis comedication in severely malnourished HIV-infected children. LPV pharmacokinetics was found to be highly variable and bioavailability greatly reduced, resulting in a high CL estimate in this population. The role of LPV dose adjustment should be further evaluated in severely malnourished children initiating ART.
在发展中国家,营养不良仍然是艾滋病病毒治疗(ART)开始时的常见临床综合征。由于营养不良和营养恢复期间的生理变化可能会影响抗逆转录病毒药物的药代动力学。
患有严重急性营养不良的 HIV 感染儿童被随机分配到早期或延迟开始洛匹那韦(LPV)/利托那韦、阿巴卡韦和拉米夫定,使用世界卫生组织体重带剂量图表。在第 1 天和第 14 天测量 LPV 浓度。此后,患者随访至第 48 周。使用 NONMEM v7.3 描述 LPV 的群体药代动力学。筛选协变量以评估其对 LPV 药代动力学的影响,并评估药代动力学变异性与治疗结果之间的关系。
从 62 名 0.1-3.9 岁(中位数:0.9 岁)的儿科患者中收集了 502 个 LPV 浓度。20 名患者接受了利福平为基础的抗结核治疗和“超级强化”LPV/利托那韦治疗。LPV 处置由一个具有一级消除的单室模型很好地描述。无论是早期还是延迟 ART 随机化、结核病合并用药还是人体测量学测量都不能解释药代动力学的可变性。无脂肪质量的比例影响表观清除率(CL/F)和分布容积(Vd/F)。药代动力学暴露与 12 或 48 周时的病毒学结果或死亡没有相关性。
在严重营养不良的 HIV 感染儿童中,LPV 药代动力学受无脂肪质量的影响,而不受 ART 起始时间或结核病合并用药的影响。在该人群中,LPV 药代动力学发现高度可变,生物利用度大大降低,导致 CL 估计值较高。在开始 ART 的严重营养不良儿童中,应进一步评估 LPV 剂量调整的作用。