Department of Pharmacy and Pharmacology, Antoni van Leeuwenhoek Hospital/The Netherlands Cancer Institute, PO Box 90440, 1006 BK, Amsterdam, The Netherlands.
Scientific Information Service, Antoni van Leeuwenhoek Hospital/The Netherlands Cancer Institute, Amsterdam, The Netherlands.
Clin Pharmacokinet. 2021 Sep;60(9):1149-1169. doi: 10.1007/s40262-021-01031-z. Epub 2021 Jun 1.
Patients affected by poverty-related infectious diseases (PRDs) are disproportionally affected by malnutrition. To optimize treatment of patients affected by PRDs, we aimed to assess the influence of malnutrition associated with PRDs on drug pharmacokinetics, by way of a systematic review.
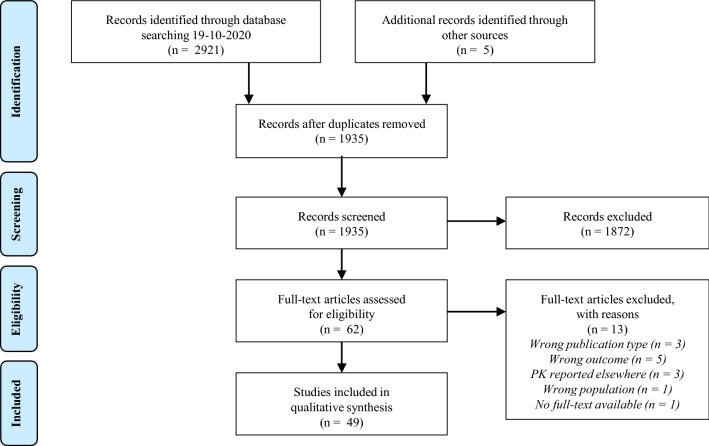
A systematic review was performed on the effects of malnourishment on the pharmacokinetics of drugs to treat PRDs, including HIV, tuberculosis, malaria, and neglected tropical diseases.
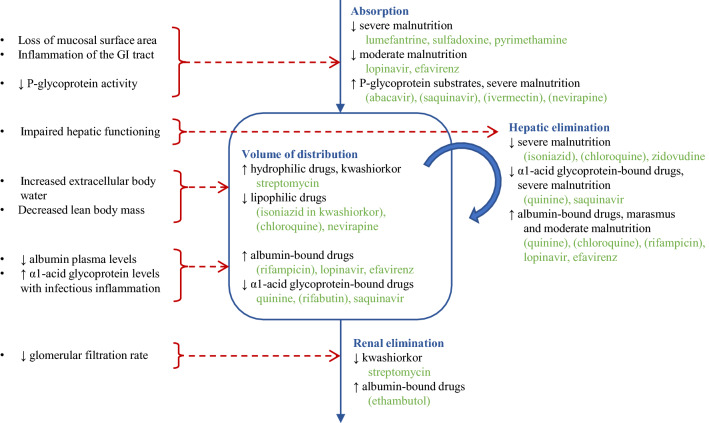
In 21/29 PRD drugs included in this review, pharmacokinetics were affected by malnutrition. Effects were heterogeneous, but trends were observed for specific classes of drugs and different types and degrees of malnutrition. Bioavailability of lumefantrine, sulfadoxine, pyrimethamine, lopinavir, and efavirenz was decreased in severely malnourished patients, but increased for the P-glycoprotein substrates abacavir, saquinavir, nevirapine, and ivermectin. Distribution volume was decreased for the lipophilic drugs isoniazid, chloroquine, and nevirapine, and the α1-acid glycoprotein-bound drugs quinine, rifabutin, and saquinavir. Distribution volume was increased for the hydrophilic drug streptomycin and the albumin-bound drugs rifampicin, lopinavir, and efavirenz. Drug elimination was decreased for isoniazid, chloroquine, quinine, zidovudine, saquinavir, and streptomycin, but increased for the albumin-bound drugs quinine, chloroquine, rifampicin, lopinavir, efavirenz, and ethambutol. Clinically relevant effects were mainly observed in severely malnourished and kwashiorkor patients.
Malnutrition-related effects on pharmacokinetics potentially affect treatment response, particularly for severe malnutrition or kwashiorkor. However, pharmacokinetic knowledge is lacking for specific populations, especially patients with neglected tropical diseases and severe malnutrition. To optimize treatment in these neglected subpopulations, adequate pharmacokinetic studies are needed, including severely malnourished or kwashiorkor patients.
受贫困相关传染病(PRD)影响的患者受到营养不良的不成比例影响。为了优化受 PRD 影响的患者的治疗效果,我们旨在通过系统评价评估营养不良与 PRD 相关药物的药代动力学之间的关系。
对治疗 PRD(包括 HIV、结核病、疟疾和被忽视的热带病)的药物的营养不良对药代动力学的影响进行了系统评价。
在本综述中纳入的 21/29 种 PRD 药物中,药代动力学受到营养不良的影响。这些影响具有异质性,但在特定药物类别和不同类型和程度的营养不良中观察到了趋势。在严重营养不良的患者中,青蒿琥酯、磺胺多辛、乙胺嘧啶、洛匹那韦和依非韦伦的生物利用度降低,但阿巴卡韦、沙奎那韦、奈韦拉平、伊维菌素等 P-糖蛋白底物的生物利用度增加。脂溶性药物异烟肼、氯喹和奈韦拉平以及与α1-酸性糖蛋白结合的药物奎宁、利福布汀和沙奎那韦的分布容积减少。亲水性药物链霉素和与白蛋白结合的药物利福平、洛匹那韦和依非韦伦的分布容积增加。异烟肼、氯喹、奎宁、齐多夫定、沙奎那韦和链霉素的药物消除减少,但与白蛋白结合的药物奎宁、氯喹、利福平、洛匹那韦、依非韦伦和乙胺丁醇的药物消除增加。临床相关的影响主要在严重营养不良和夸希奥科营养不良患者中观察到。
药代动力学方面的营养不良相关影响可能会影响治疗反应,特别是在严重营养不良或夸希奥科营养不良的情况下。然而,特定人群的药代动力学知识缺乏,尤其是患有被忽视的热带病和严重营养不良的患者。为了优化这些被忽视的亚人群的治疗效果,需要进行充分的药代动力学研究,包括严重营养不良或夸希奥科营养不良的患者。