Sean N Parker Center for Allergy and Asthma Research, Stanford University School of Medicine, Stanford, CA, USA.
Sean N Parker Center for Allergy and Asthma Research, Stanford University School of Medicine, Stanford, CA, USA; Quantitative Sciences Unit, Stanford University School of Medicine, Stanford, CA, USA.
Lancet Gastroenterol Hepatol. 2018 Feb;3(2):85-94. doi: 10.1016/S2468-1253(17)30392-8. Epub 2017 Dec 12.
Despite progress in single food oral immunotherapy, there is little evidence concerning the safety and efficacy of treating individuals with multiple food (multifood) allergies. We did a pilot study testing whether anti-IgE (omalizumab) combined with multifood oral immunotherapy benefited multifood allergic patients.
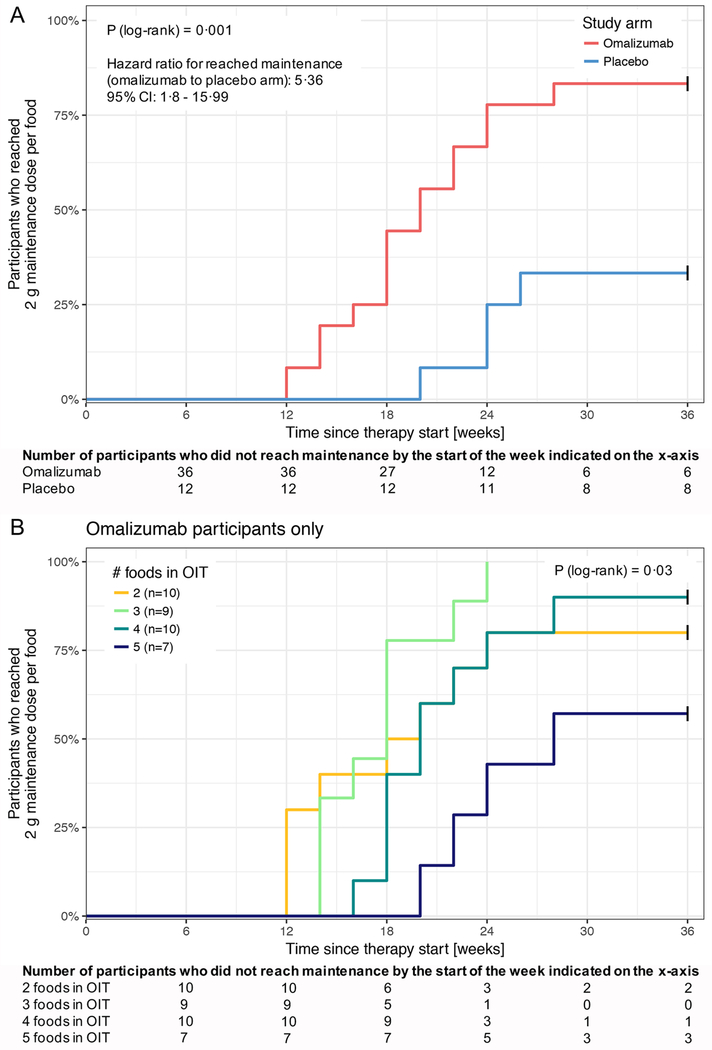
We did a blinded, phase 2 clinical trial at Stanford University. We enrolled participants, aged 4-15 years, with multifood allergies validated by double-blind, placebo-controlled food challenges to their offending foods. Inclusion criteria included a positive skin prick test of 6 mm or more (wheal diameter, above the negative control), a food-specific serum IgE concentration of more than 4 kU/L for each food, or both, and a positive double-blind, placebo-controlled food challenge at 500 mg or less of food protein. Exclusion criteria included eosinophilic oesophagitis and severe asthma. Participants were randomised (3:1) with a block size of four, to receive multifood oral immunotherapy to two to five foods, together with omalizumab (n=36) or placebo (n=12). 12 individuals who fulfilled the same inclusion and exclusion criteria were included as controls. These individuals were not randomised and received neither omalizumab nor oral immunotherapy. Omalizumab or placebo was administered subcutaneously for 16 weeks, with oral immunotherapy starting at week 8, and was stopped 20 weeks before the exit double-blind, placebo-controlled food challenge at week 36. The primary endpoint was the proportion of participants who passed double-blind, placebo-controlled food challenges to at least two of their offending foods. This completed trial is registered with ClinicalTrials.gov, number NCT02643862.
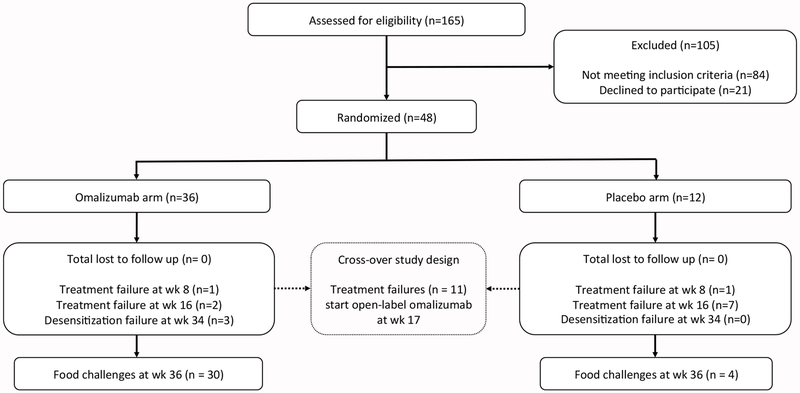
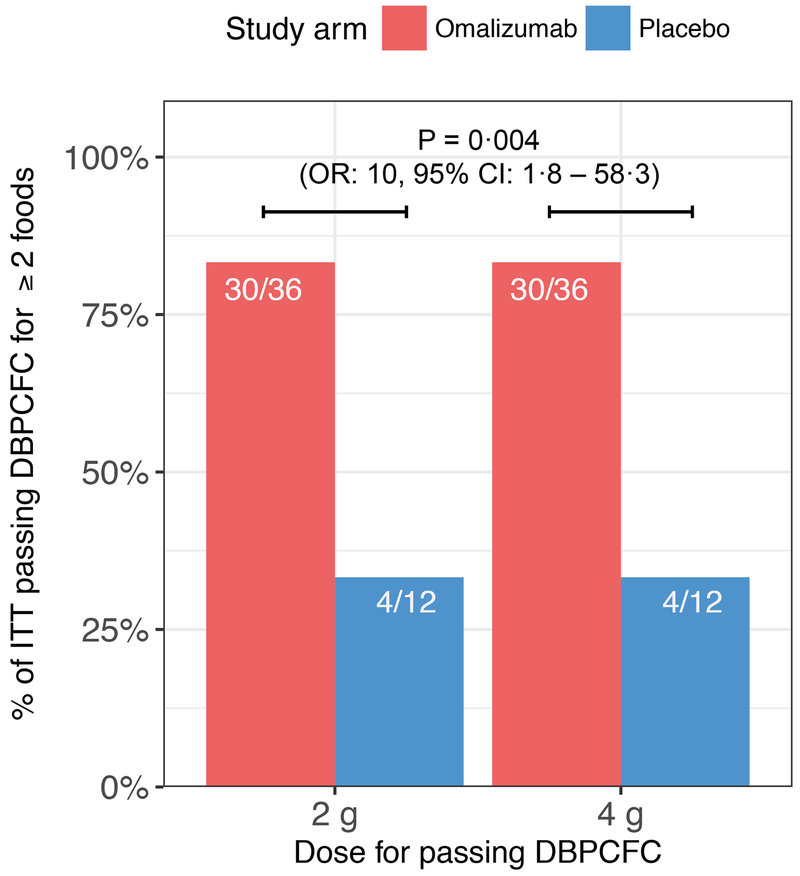
Between March 25, 2015, and Aug 18, 2016, 165 participants were assessed for eligibility, of whom 84 did not meet the inclusion criteria and 21 declined to participate. We enrolled and randomised 48 eligible participants and the remaining 12 patients were included as nonrandomised, untreated controls. At week 36, a significantly greater proportion of the omalizumab-treated (30 [83%] of 36) versus placebo (four [33%] of 12) participants passed double-blind, placebo-controlled food challenges to 2 g protein for two or more of their offending foods (odds ratio 10·0, 95% CI 1·8-58·3, p=0·0044). All participants completed the study. There were no serious or severe (grade 3 or worse) adverse events. Participants in the omalizumab group had a significantly lower median per-participant percentage of oral immunotherapy doses associated with any adverse events (27% vs 68%; p=0·0082). The most common adverse events in both groups were gastrointestinal events.
In multifood allergic patients, omalizumab improves the efficacy of multifood oral immunotherapy and enables safe and rapid desensitisation.
US National Institutes of Health (NIH).
尽管在单一食物口服免疫治疗方面取得了进展,但对于治疗多种食物过敏(多食物过敏)患者的安全性和疗效,几乎没有证据。我们进行了一项试点研究,以测试抗 IgE(奥马珠单抗)联合多食物口服免疫疗法是否对多食物过敏患者有益。
我们在斯坦福大学进行了一项盲法、2 期临床试验。我们招募了年龄在 4-15 岁之间的参与者,这些参与者的多食物过敏已通过对其过敏原食物进行双盲、安慰剂对照食物挑战得到证实。纳入标准包括:阳性皮肤点刺试验(皮丘直径大于阴性对照 6 毫米);每种食物的特异性血清 IgE 浓度大于 4 kU/L;或两者兼有;以及在 500 毫克或更少的食物蛋白时进行阳性双盲、安慰剂对照食物挑战。排除标准包括嗜酸性食管炎和严重哮喘。参与者按 3:1 的比例随机分组(每组 4 个块),接受 2-5 种食物的多食物口服免疫治疗,同时接受奥马珠单抗(n=36)或安慰剂(n=12)治疗。12 名符合相同纳入和排除标准的个体被纳入对照组。这些个体未随机分组,未接受奥马珠单抗或口服免疫治疗。奥马珠单抗或安慰剂每 2 周皮下注射 16 周,口服免疫治疗从第 8 周开始,并在第 36 周退出时的双盲、安慰剂对照食物挑战前 20 周停止。主要终点是至少有两名参与者通过双盲、安慰剂对照食物挑战来耐受至少两种过敏原食物的比例。这项完成的试验在 ClinicalTrials.gov 上注册,编号为 NCT02643862。
在 2015 年 3 月 25 日至 2016 年 8 月 18 日期间,对 165 名参与者进行了资格评估,其中 84 名不符合纳入标准,21 名拒绝参与。我们招募并随机分配了 48 名合格的参与者,其余 12 名患者作为非随机、未经治疗的对照组。在第 36 周时,接受奥马珠单抗治疗(36 名中的 30 名,83%)的参与者与接受安慰剂治疗(12 名中的 4 名,33%)相比,通过双盲、安慰剂对照食物挑战来耐受 2 克蛋白的两种或两种以上过敏原食物的比例显著更高(比值比 10.0,95%CI 1.8-58.3,p=0.0044)。所有参与者均完成了研究。没有发生严重或严重(3 级或更高级别)不良事件。奥马珠单抗组参与者的口服免疫治疗相关不良事件的中位每人百分比明显较低(27% vs 68%;p=0.0082)。两组中最常见的不良事件是胃肠道事件。
在多食物过敏患者中,奥马珠单抗可提高多食物口服免疫治疗的疗效,并实现安全、快速脱敏。
美国国立卫生研究院(NIH)。