Paepegaey Anne-Cécile, Salenave Sylvie, Kamenicky Peter, Maione Luigi, Brailly-Tabard Sylvie, Young Jacques, Chanson Philippe
Service d'Endocrinologie et des Maladies de la Reproduction and Centre de Référence des Maladies Endocriniennes Rares de la Croissance, and.
INSERM 1185, Faculté de Médecine Paris Sud, Université Paris-Saclay, Kremlin-Bicêtre, F-94276, France.
J Endocr Soc. 2017 Feb 16;1(3):221-230. doi: 10.1210/js.2017-00038. eCollection 2017 Mar 1.
Cabergoline (CAB) is very effective in the treatment of macroprolactinomas, but there are few data on the CAB dose necessary to achieve and maintain normal prolactin (PRL) levels.
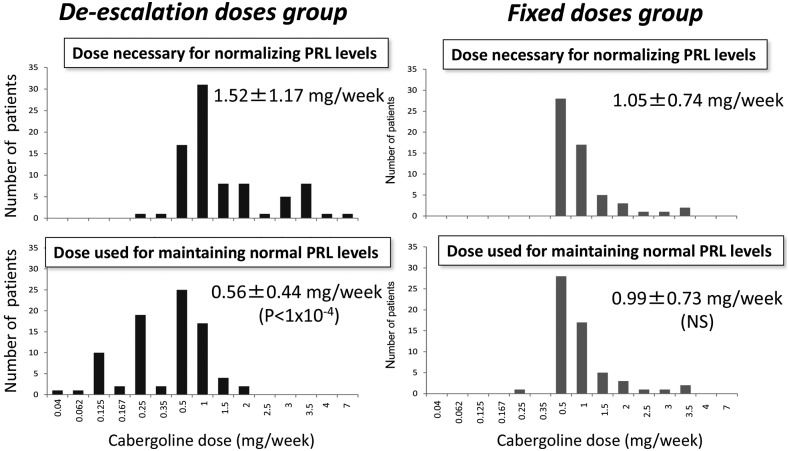
We retrospectively studied 260 patients. CAB was introduced at a mean dose of 0.83 ± 0.52 mg/wk. When the PRL level had normalized, the patient's physician chose to either maintain the CAB dose (fixed-dose group) or to taper it (de-escalation group) until the minimal effective dose required to maintain a normal PRL level was established.
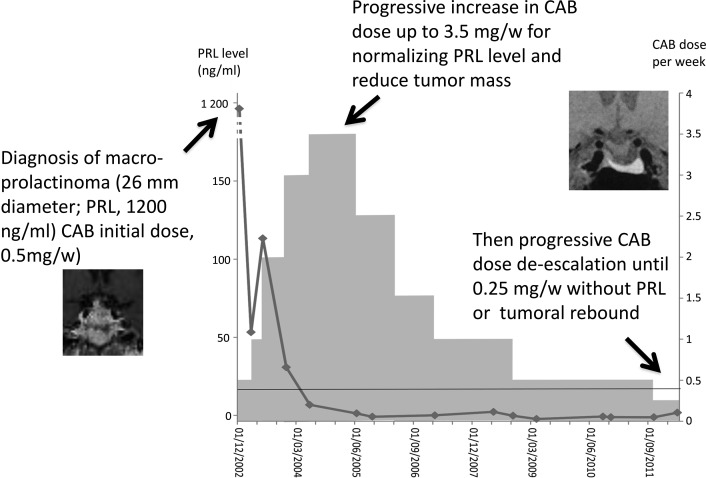
PRL normalized in 157 patients (60.8%) during CAB treatment. CAB de-escalation was attempted in 84 (53.5%) of these 157 patients and was successful in 77 (91.7%) cases. The mean CAB dose was reduced from 1.52 ± 1.17 mg/wk to 0.56 ± 0.44 mg/wk at the last visit ( < 1 × 10). De-escalation was also possible in some "CAB-resistant" patients, namely those requiring ≥2 mg/wk to normalize PRL. CAB de-escalation had no negative long-term effect on tumor size. At the last visit, maximal diameter was 8.8 ± 8.8 mm in the de-escalation group and 13.4 ± 8.5 mm in the fixed-dose group ( < 0.01).
In patients with macroprolactinomas, the CAB dosage required to maintain a normal PRL level long term is lower than the initial dosage necessary to normalize the PRL level. After PRL normalization, CAB tapering was almost always successful, even when very high initial doses were necessary. CAB tapering does not undermine tumor control and may attenuate the potential adverse effects of CAB, which appear to be dependent on the cumulative dose.
卡麦角林(CAB)在治疗大泌乳素瘤方面非常有效,但关于达到并维持正常泌乳素(PRL)水平所需的卡麦角林剂量的数据较少。
我们对260例患者进行了回顾性研究。卡麦角林的起始平均剂量为0.83±0.52mg/周。当PRL水平恢复正常后,患者的医生选择维持卡麦角林剂量(固定剂量组)或逐渐减量(减量组),直到确定维持正常PRL水平所需的最小有效剂量。
在卡麦角林治疗期间,157例患者(60.8%)的PRL恢复正常。在这157例患者中,84例(53.5%)尝试了卡麦角林减量,77例(91.7%)成功。末次随访时,卡麦角林的平均剂量从1.52±1.17mg/周降至0.56±0.44mg/周(<1×10)。一些“卡麦角林抵抗”患者,即那些需要≥2mg/周才能使PRL恢复正常的患者,也可以进行减量。卡麦角林减量对肿瘤大小没有长期负面影响。末次随访时,减量组的最大直径为8.8±8.8mm,固定剂量组为13.4±8.5mm(<0.01)。
对于大泌乳素瘤患者,长期维持正常PRL水平所需的卡麦角林剂量低于使PRL水平恢复正常所需的初始剂量。PRL恢复正常后,卡麦角林减量几乎总是成功的,即使最初需要非常高的剂量。卡麦角林减量不会影响肿瘤控制,并且可能减轻卡麦角林的潜在不良反应,这些不良反应似乎取决于累积剂量。