Bohlouli Babak, Jackson Terri, Tonelli Marcello, Hemmelgarn Brenda, Klarenbach Scott
Department of Medicine, University of Alberta, 11-112R Clinical Sciences Building, 8440-112 Street, Edmonton, AB, T6G2G3, Canada.
University of Melbourne, Northern Clinical Research Centre, The Northern Hospital, 185 Cooper St, Epping, VIC, 3076, Australia.
BMC Nephrol. 2017 Dec 28;18(1):375. doi: 10.1186/s12882-017-0784-2.
Patients with CKD are at increased risk of potentially preventable hospital acquired complications (HACs). Understanding the economic consequences of preventable HACs, may define the scope and investment of initiatives aimed at prevention.
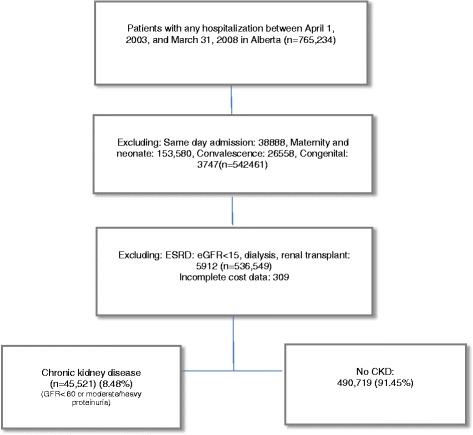
Adult patients hospitalized from April, 2003 to March, 2008 in Alberta, Canada comprised the study cohort. Healthcare costs were determined and categorized into 'index hospitalization' including hospital cost and in-hospital physician claims, and 'post discharge' including ambulatory care cost, physician claims, and readmission costs from discharge to 90 days. Multivariable regression was used to estimate the incremental healthcare costs associated with potentially preventable HACs.
In fully adjusted models, the median incremental index hospitalization cost was CAN-$6169 (95% CI; 6003-6336) in CKD patients with ≥1 potentially preventable HACs, compared with those without. Post-discharge incremental costs were 1471(95% CI; 844-2099) in those patients with CKD who developed potentially preventable HACs within 90 days after discharge compared with patients without potentially preventable HACs. Additionally, the incremental costs associated with ≥1 potentially preventable HACs within 90 days from admission in patients with CKD were $7522 (95% CI; 7219-7824). A graded relation of the incremental costs was noted with the increasing number of complications. In patients without CKD but with ≥1 preventable HACs incremental costs within 90 days from hospital admission was $6688 (95% CI: 6612-6723).
Potentially preventable HACs are associated with substantial increases in healthcare costs in people with CKD. Investment in implementing targeted strategies to reduce HACs may have a significant benefit for patient and health system outcomes.
慢性肾脏病(CKD)患者发生潜在可预防的医院获得性并发症(HACs)的风险增加。了解可预防的HACs的经济后果,可能有助于确定预防措施的范围和投入。
研究队列包括2003年4月至2008年3月在加拿大艾伯塔省住院的成年患者。确定医疗费用并分为“首次住院”(包括住院费用和住院期间医生费用)和“出院后”(包括门诊护理费用、医生费用以及出院至90天内的再入院费用)。采用多变量回归来估计与潜在可预防的HACs相关的增量医疗费用。
在完全调整的模型中,与无潜在可预防HACs的CKD患者相比,有≥1种潜在可预防HACs的CKD患者首次住院增量费用中位数为6169加元(95%CI:6003 - 6336)。与无潜在可预防HACs的患者相比,出院后90天内发生潜在可预防HACs的CKD患者出院后增量费用为1471加元(95%CI:844 - 2099)。此外,CKD患者入院后90天内发生≥1种潜在可预防HACs的增量费用为7522美元(95%CI:7219 - 7824)。随着并发症数量的增加,增量费用呈分级关系。在无CKD但有≥1种可预防HACs的患者中,入院后90天内的增量费用为6688美元(95%CI:6612 - 6723)。
潜在可预防的HACs与CKD患者的医疗费用大幅增加相关。投资实施有针对性的策略以减少HACs可能对患者和卫生系统结局产生重大益处。