Bisui Bikash, Samanta Swastika, Ghoshmaulik Sumanta, Banerjee Amit, Ghosh Tirtha R, Sarkar Suman
Department of Anaesthesiology and Critical Care, BS Medical College, Bankura, West Bengal, India.
Department of Anaesthesiology and Critical Care, Burdwan Medical College and Hospital, Burdwan, West Bengal, India.
Anesth Essays Res. 2017 Oct-Dec;11(4):981-986. doi: 10.4103/aer.AER_55_17.
Brachial plexus block is effective with good postoperative analgesia in upper limb surgery has gained importance as it safe, low cost, and maintains stable hemodynamics intraoperatively. To decrease the onset time and prolong the duration of nerve block bicarbonate, opioids (morphine, fentanyl, etc.), sympathomimetic agents (epinephrine, phenylephrine, etc.), α-2 agonists (clonidine and dexmedetomidine), calcium channel blocker (verapamil), magnesium sulfate, etc., were studied with local anesthetics and their isomers. For their sedative, analgesic, perioperative sympatholytic, and cardiovascular stabilizing effects with reduced anesthetic requirements, α-2 adrenergic receptor agonists, such as more potent and highly selective dexmedetomidine, have been the focus of interest for regional anesthesia. Intravenous dexmedetomidine infusion resulted in significant opioid-sparing effects as well as a decrease in inhalational anesthetic requirements. Animal studies proved that dexmedetomidine enhances sensory and motor blockade along with increased duration of analgesia. In humans, dexmedetomidine has also shown to prolong the duration of block and postoperative analgesia when added to local anesthetic in various regional blocks. Bupivacaine, the widely used local anesthetic in regional anesthesia, is available in a commercial preparation as a racemic mixture (50:50) of its two enantiomers: levobupivacaine, S (-) isomer and dextrobupivacaine, R (+) isomer. Severe central nervous system and cardiovascular adverse reactions reported in the literature after inadvertent intravascular injection or intravenous regional anesthesia have been linked to the R (+) isomer of bupivacaine. The levorotatory isomers were shown to have a safer pharmacological profile with less cardiac and neurotoxic adverse effects. The decreased toxicity of levobupivacaine is attributed to its faster protein binding rate. The pure S (-) enantiomers of bupivacaine, i.e., ropivacaine and levobupivacaine were thus introduced into the clinical anesthesia practice. Such an increased usage mandates the documentation of evidence-based literature with regard to risk and safety concerns as well as clinical issues related to levobupivacaine. This study is designed to assess the efficacy of adding dexmedetomidine to levobupivacaine during placement of supraclavicular brachial plexus blockade.
This prospective observational double-blinded study was conducted over a 1-year period among randomly selected seventy ( = 35) American Society of Anesthesiologists Classes I and II patients of ages between 18 and 60 years of both sexes scheduled to undergo upper limb surgery. With nerve locator, levobupivacaine (0.5%) 28 ml and 2 ml normal saline for Group L and levobupivacaine (0.5%) 28 ml and 0.75 μg/kg dexmedetomidine made up a solution of 2 ml, for Group D, a total 30 ml will be injected locally, in both the groups. Onset and duration of sensory and motor block will be assessed.
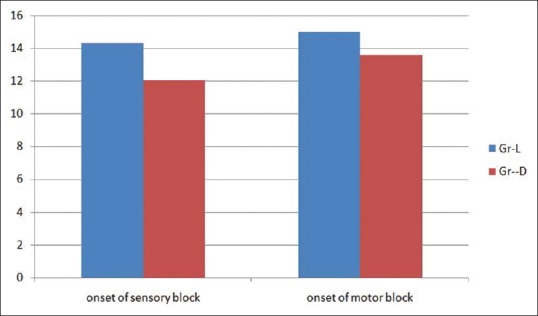
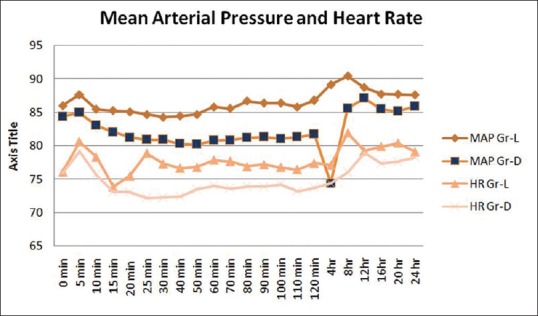
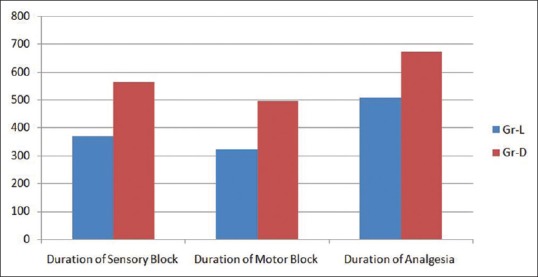
One patient in Group L and two patients in Group D failed to achieve block within 30 min. Those three patients were then excluded from the analysis. Hence, the analysis was done by taking 34 patients in Group L and 33 patients in Group D. Onset of sensory and motor block was earlier in Group D (12.03 ± 0.85 and 13.58 ± 0.97) than Group L (14.32 ± 1.15 and 15 ± 0.98), and the difference is statistically significant ( < 0.0001). Duration of sensory and motor block was longer in Group D (563.94 ± 15.60 and 495.15 ± 10.34) than Group L (368.53 ± 9.89 and 321.47 ± 7.84), and the difference is also statistically significant ( < 0.0001). Duration of analgesia was longer in Group D (672.12 ± 11.39) than Group L (506.47 ± 9.497), and the difference is statistically significant ( < 0.0001). Heart rate and mean arterial pressure were well maintained within the presumed range of significant variation, i.e., 20% from baseline, though at some point of time, intergroup comparison was statistically significant. Visual analog scale score compared at the time for administration of rescue analgesic between the groups come out to be statistically significant.
Addition of 0.75 μg/kg dexmedetomidine to 0.5% levobupivacaine for supraclavicular plexus block shortens sensory and motor block onset time and extends sensory block, motor block, and analgesia duration.
臂丛神经阻滞在上肢手术中能有效提供良好的术后镇痛效果,因其安全、成本低且术中能维持稳定的血流动力学而备受重视。为缩短神经阻滞的起效时间并延长其持续时间,人们研究了将碳酸氢盐、阿片类药物(吗啡、芬太尼等)、拟交感神经药(肾上腺素、去氧肾上腺素等)、α -2激动剂(可乐定和右美托咪定)、钙通道阻滞剂(维拉帕米)、硫酸镁等与局部麻醉药及其异构体联合使用。α -2肾上腺素能受体激动剂,如更有效且高度选择性的右美托咪定,因其镇静、镇痛、围手术期抗交感神经和心血管稳定作用以及降低麻醉需求,一直是区域麻醉关注的焦点。静脉输注右美托咪定可产生显著的阿片类药物节省效应,并减少吸入麻醉药的需求。动物研究证明,右美托咪定可增强感觉和运动阻滞,并延长镇痛持续时间。在人体中,右美托咪定添加到各种区域阻滞的局部麻醉药中时,也显示出能延长阻滞持续时间和术后镇痛时间。布比卡因是区域麻醉中广泛使用的局部麻醉药,其市售制剂为两种对映体(左旋布比卡因,S(-)异构体和右旋布比卡因,R(+)异构体)的外消旋混合物(50:50)。文献报道布比卡因无意血管内注射或静脉区域麻醉后出现的严重中枢神经系统和心血管不良反应与布比卡因的R(+)异构体有关。左旋异构体显示出具有更安全的药理学特征及较少的心毒性和神经毒性不良反应。左旋布比卡因毒性降低归因于其更快的蛋白结合率。因此,布比卡因纯S(-)对映体,即罗哌卡因和左旋布比卡因被引入临床麻醉实践中。这种使用增加要求记录关于左旋布比卡因的风险和安全问题以及临床问题的确凿文献。本研究旨在评估在锁骨上臂丛神经阻滞时将右美托咪定添加到左旋布比卡因中的效果。
本前瞻性观察性双盲研究在1年期间对随机选择的70例(每组35例)年龄在18至60岁之间、拟行上肢手术的美国麻醉医师协会I级和II级男女患者进行。使用神经定位仪,L组给予28 ml 0.5%左旋布比卡因和2 ml生理盐水,D组给予28 ml 0.5%左旋布比卡因和0.75 μg/kg右美托咪定配制成2 ml溶液,两组均局部注射共30 ml。评估感觉和运动阻滞的起效时间和持续时间。
L组1例患者和D组2例患者在30分钟内未达到阻滞效果。这3例患者随后被排除在分析之外。因此,分析是在L组34例患者和D组33例患者中进行的。D组感觉和运动阻滞的起效时间(12.03±0.85和13.58±0.97)比L组(14.32±1.15和15±0.98)更早,差异具有统计学意义(P<0.0001)。D组感觉和运动阻滞的持续时间(563.94±15.60和495.15±10.34)比L组(368.53±9.89和321.47±7.84)更长,差异也具有统计学意义(P<0.0001)。D组镇痛持续时间(672.·12±11.39)比L组(506.47±9.497)更长,差异具有统计学意义(P<0.0001)。心率和平均动脉压在假定的显著变化范围内(即距基线20%)得到良好维持,尽管在某些时间点,组间比较具有统计学意义。两组间在给予补救性镇痛时的视觉模拟评分比较具有统计学意义。
在0.5%左旋布比卡因中添加0.75 μg/kg右美托咪定用于锁骨上神经阻滞可缩短感觉和运动阻滞的起效时间,并延长感觉阻滞、运动阻滞和镇痛的持续时间。