Tang Kunlong, Wang Liang, Yang Zhongyuan, Sui Yingying, Li Liming, Huang Yuting, Gao Peng
Tianjin Medical University General Hospital, Tianjin, China.
Sun Yat-sen University Cancer Center, Guangzhou, China.
Oncotarget. 2017 Aug 31;8(62):106113-106120. doi: 10.18632/oncotarget.20597. eCollection 2017 Dec 1.
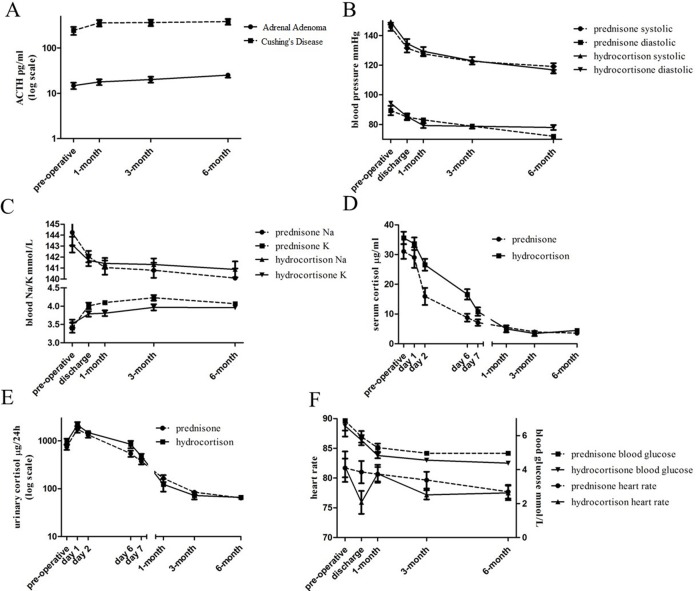
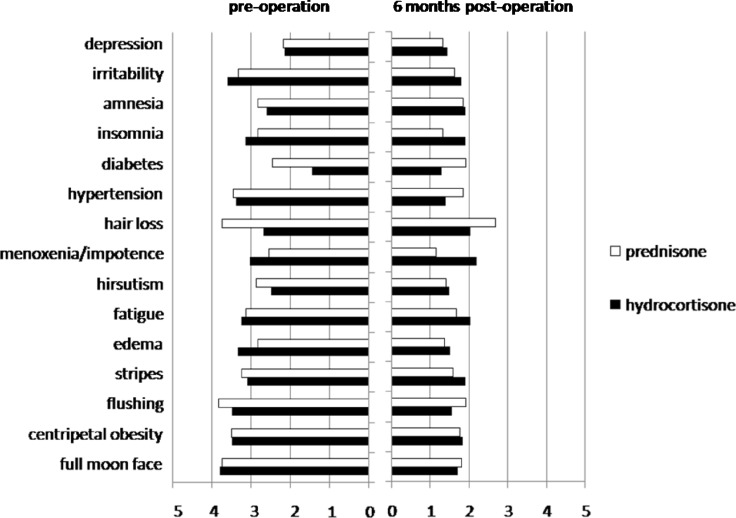
Cushing's syndrome requires glucocorticoid replacement following adrenalectomy. Based on a simplified glucocorticoid therapy scheme and the peri-operative observation, we investigated its efficacy and safety up to 6 months post-adrenalectomy in this cohort study. We found the adrenocorticotropic hormone (ACTH) levels were normal post-adrenalectomy, and sufficient to stimulate the recovery of the dystrophic adrenal cortex, thus exogenous supplemental ACTH might not be necessary. Patients were grouped by oral reception of either hydrocortisone or prednisone since day 2 post-adrenalectomy. Both groups had similar baseline responses to adrenalectomy, regarding the correction of hypertension (10/15 vs.12/19), hyperglycemia (6/11 vs. 7/10), and hypokalemia (12/12 vs. 11/11). Most patients lost weight (17/20 vs. 20/22). Both groups reported significant improvement in a subjective evaluation questionnaire. Hydrocortisone showed advantages over prednisone in improving liver function (7/8 vs. 2/7, = 0.035), but also caused significant lower extremety edema ( = 0.034). Both groups developed adrenal insufficiency (AI) during glucocorticoid withdrawal, with no significant difference regarding the incidence rate (7/20 vs. 10/22) or severity. Most AI symptoms were relieved by resuming the prior oral doses, while two severe cases were hospitalized. The withdrawal process may last longer time for hydrocortisone than prednisone. In conclusion, our data supports the use of both hydrocortisone and prednisone in the glucocorticoid replacement therapy post-adrenalectomy for patients of adrenal adenoma or Cushing's disease. Hydrocortisone showed advantages over prednisone in improving liver function, and prednisone exhibited significantly lower risk of edema.
库欣综合征患者在肾上腺切除术后需要进行糖皮质激素替代治疗。基于简化的糖皮质激素治疗方案和围手术期观察,我们在这项队列研究中调查了肾上腺切除术后6个月内其疗效和安全性。我们发现肾上腺切除术后促肾上腺皮质激素(ACTH)水平正常,足以刺激营养不良的肾上腺皮质恢复,因此可能无需外源性补充ACTH。自肾上腺切除术后第2天起,患者按口服氢化可的松或泼尼松分组。两组在肾上腺切除术后的基线反应相似,在高血压纠正方面(10/15 vs.12/19)、高血糖方面(6/11 vs. 7/10)和低钾血症方面(12/12 vs. 11/11)。大多数患者体重减轻(17/20 vs. 20/22)。两组在主观评估问卷中均报告有显著改善。氢化可的松在改善肝功能方面优于泼尼松(7/8 vs. 2/7,P = 0.035),但也导致下肢明显水肿(P = 0.034)。两组在糖皮质激素撤减期间均出现肾上腺功能不全(AI),发病率(7/20 vs. 10/22)或严重程度无显著差异。大多数AI症状通过恢复先前口服剂量得到缓解,而有两例严重病例住院治疗。氢化可的松的撤减过程可能比泼尼松持续时间更长。总之,我们的数据支持在肾上腺腺瘤或库欣病患者肾上腺切除术后的糖皮质激素替代治疗中使用氢化可的松和泼尼松。氢化可的松在改善肝功能方面优于泼尼松,而泼尼松出现水肿的风险显著较低。