Gastrointestinal Medical Oncology Division, National Cancer Center Hospital, Tokyo, Japan.
Division of Gastroenterology, Chiba Cancer Center, Chiba, Japan.
Ann Oncol. 2018 Mar 1;29(3):624-631. doi: 10.1093/annonc/mdx816.
Combination therapy with oral fluoropyrimidine and irinotecan has not yet been established as first-line treatment of metastatic colorectal cancer (mCRC). We carried out a randomized, open-label, phase III trial to determine whether S-1 and irinotecan plus bevacizumab is noninferior to mFOLFOX6 or CapeOX plus bevacizumab in terms of progression-free survival (PFS).
Patients from 53 institutions who had previously untreated mCRC were randomly assigned (1 : 1) to receive either mFOLFOX6 or CapeOX plus bevacizumab (control group) or S-1 and irinotecan plus bevacizumab (experimental group; a 3-week regimen: intravenous infusions of irinotecan 150 mg/m2 and bevacizumab 7.5 mg/kg on day 1, oral S-1 80 mg/m2 twice daily for 2 weeks, followed by a 1-week rest; or a 4-week regimen: irinotecan 100 mg/m2 and bevacizumab 5 mg/kg on days 1 and 15, S-1 80 mg/m2 twice daily for 2 weeks, followed by a 2-week rest). The primary end point was PFS. The noninferiority margin was 1.25; noninferiority would be established if the upper limit of the 95% confidence interval (CI) for the hazard ratio (HR) of the control group versus the experimental group was less than this margin.
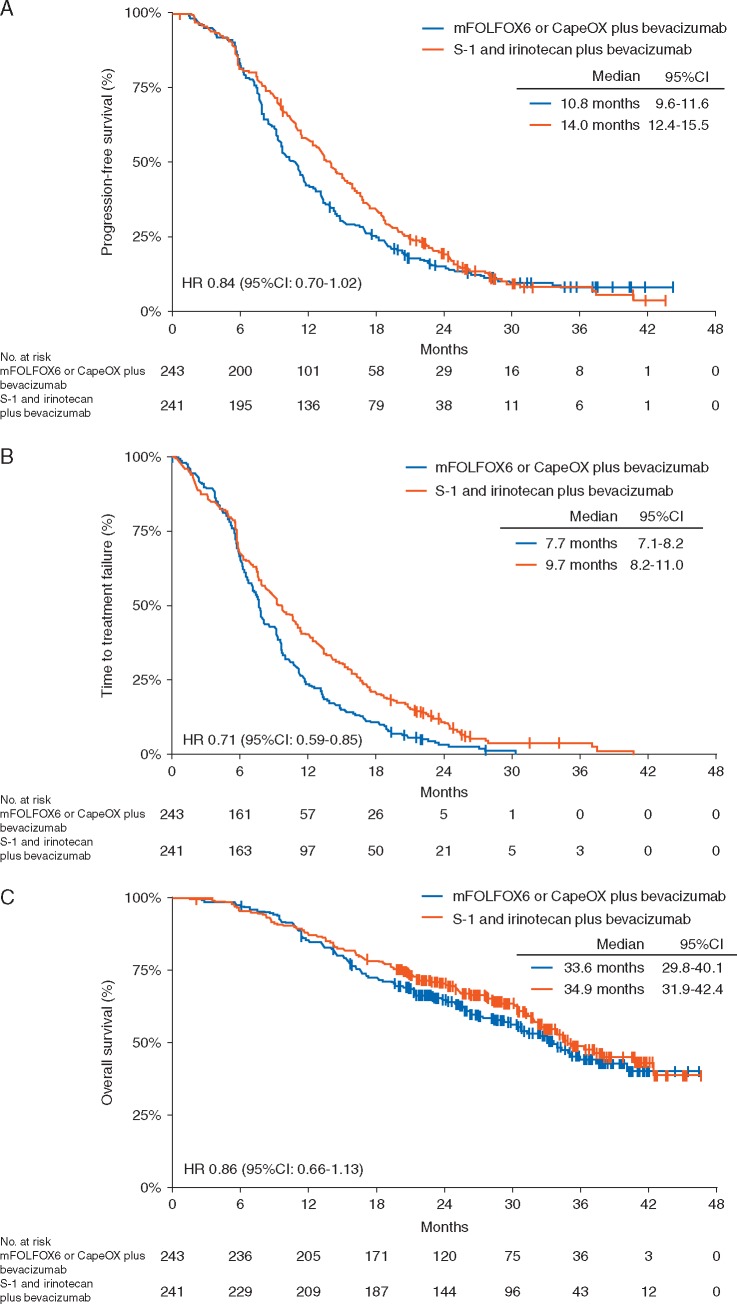
Between June 2012 and September 2014, 487 patients underwent randomization. Two hundred and forty-three patients assigned to the control group and 241 assigned to the experimental group were included in the primary analysis. Median PFS was 10.8 months (95% CI 9.6-11.6) in the control group and 14.0 months (95% CI 12.4-15.5) in the experimental group (HR 0.84, 95% CI 0.70-1.02; P < 0.0001 for noninferiority, P = 0.0815 for superiority). One hundred and fifty-seven patients (64.9%) in the control group and 140 (58.6%) in the experimental group had adverse events of grade 3 or higher.
S-1 and irinotecan plus bevacizumab is noninferior to mFOLFOX6 or CapeOX plus bevacizumab with respect to PFS as first-line treatment of mCRC and could be a new standard treatment.
UMIN000007834.
口服氟嘧啶和伊立替康联合治疗转移性结直肠癌(mCRC)尚未被确立为一线治疗。我们进行了一项随机、开放标签、III 期试验,以确定 S-1 和伊立替康联合贝伐珠单抗是否不劣于 mFOLFOX6 或 CapeOX 联合贝伐珠单抗在无进展生存期(PFS)方面。
来自 53 家机构的未经治疗的 mCRC 患者被随机分配(1:1)接受 mFOLFOX6 或 CapeOX 联合贝伐珠单抗(对照组)或 S-1 和伊立替康联合贝伐珠单抗(实验组;3 周方案:静脉注射伊立替康 150mg/m2 和贝伐珠单抗 7.5mg/kg 于第 1 天,S-1 80mg/m2 每日 2 次口服,连续 2 周,然后休息 1 周;或 4 周方案:伊立替康 100mg/m2 和贝伐珠单抗 5mg/kg 于第 1 天和第 15 天,S-1 80mg/m2 每日 2 次口服,连续 2 周,然后休息 2 周)。主要终点是 PFS。非劣效性边界为 1.25;如果对照组与实验组的风险比(HR)的 95%置信区间(CI)上限小于该边界,则可以建立非劣效性。
2012 年 6 月至 2014 年 9 月期间,有 487 名患者接受了随机分组。243 名被分配到对照组和 241 名被分配到实验组的患者被纳入主要分析。对照组的中位 PFS 为 10.8 个月(95%CI 9.6-11.6),实验组为 14.0 个月(95%CI 12.4-15.5)(HR 0.84,95%CI 0.70-1.02;P<0.0001 表示非劣效性,P=0.0815 表示优效性)。对照组中有 157 名(64.9%)患者和实验组中有 140 名(58.6%)患者发生 3 级或更高级别的不良事件。
S-1 和伊立替康联合贝伐珠单抗与 mFOLFOX6 或 CapeOX 联合贝伐珠单抗在 PFS 方面不劣于一线治疗 mCRC,并且可能成为一种新的标准治疗方法。
UMIN000007834。