Page Evaren E, Kremer Hovinga Johanna A, Terrell Deirdra R, Vesely Sara K, George James N
Department of Biostatistics and Epidemiology, College of Public Health, and.
Department of Medicine, College of Medicine, University of Oklahoma Health Sciences Center, Oklahoma City, OK; and.
Blood Adv. 2017 Apr 6;1(10):590-600. doi: 10.1182/bloodadvances.2017005124. eCollection 2017 Apr 11.
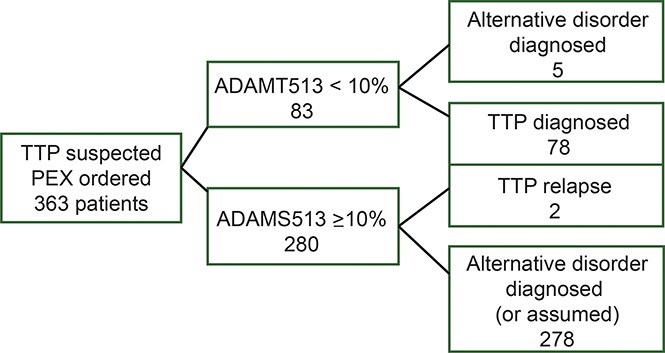
Our objective was to describe new observations from the Oklahoma Thrombotic Thrombocytopenic Purpura (TTP) Registry experience (November 1995 through December 2015) on the diagnosis of TTP along with patients' clinical features and their outcomes. Among 363 patients with an initial episode of clinically suspected TTP, the diagnosis of TTP was supported by both ADAMTS13 activity <10% and clinical features in 78 patients (21%). ADAMTS13 activity was measured in all 363 patients by 2 methods: fluorescence resonance energy transfer (FRET) and immunoblotting (IB). Sixty patients had ADAMTS13 activity <10% by both methods, 15 had ADAMTS13 <10% only by FRET, and 3 had ADAMTS13 <10% only by IB. Five patients with ADAMTS13 activity <10% by 1 method had an alternative clinical diagnosis, not TTP. Two patients with characteristic clinical features of TTP (microangiopathic hemolytic anemia and thrombocytopenia, no alternative diagnosis) and multiple relapses initially had ADAMTS13 activity >10% by both measurements. ADAMTS13 inhibitor titers were not associated with presenting features or outcomes. Microangiopathic hemolytic anemia and thrombocytopenia were not severe in all patients. Forty-seven percent of patients had no or minor neurologic abnormalities; 95% had no or minor serum creatinine abnormalities. Ten patients (13%) died, 2 before completing 1 plasma exchange (PEX); 3 deaths were attributed to PEX complications. For patients presenting after we began using rituximab in some patients (December 2003), fewer PEX treatments were required and fewer relapses occurred. Patients with their first relapse presented with higher platelet counts and hematocrits and lower lactate dehydrogenase levels and required fewer PEX treatments compared with their initial episodes.
我们的目标是描述俄克拉荷马血栓性血小板减少性紫癜(TTP)注册研究(1995年11月至2015年12月)中关于TTP诊断以及患者临床特征和预后的新观察结果。在363例初发临床疑似TTP的患者中,78例(21%)患者的ADAMTS13活性<10%且伴有临床特征,支持TTP的诊断。通过两种方法对所有363例患者进行了ADAMTS13活性检测:荧光共振能量转移(FRET)和免疫印迹法(IB)。60例患者两种方法检测的ADAMTS13活性均<10%,15例仅FRET检测显示ADAMTS13<10%,3例仅IB检测显示ADAMTS13<10%。5例通过一种方法检测ADAMTS13活性<10%的患者有其他临床诊断,而非TTP。2例具有TTP特征性临床特征(微血管病性溶血性贫血和血小板减少,无其他诊断)且多次复发的患者,最初两种检测方法显示ADAMTS13活性均>10%。ADAMTS13抑制剂滴度与临床表现或预后无关。并非所有患者的微血管病性溶血性贫血和血小板减少都很严重。47%的患者无或仅有轻微神经系统异常;95%的患者无或仅有轻微血清肌酐异常。10例患者(13%)死亡,2例在完成1次血浆置换(PEX)前死亡;3例死亡归因于PEX并发症。对于在我们开始对部分患者使用利妥昔单抗后(2003年12月)就诊的患者,所需的PEX治疗次数更少,复发次数也更少。与首次发作相比,首次复发的患者血小板计数和血细胞比容更高,乳酸脱氢酶水平更低,所需的PEX治疗次数更少。