Westwood John-Paul, Thomas Mari, Alwan Ferras, McDonald Vickie, Benjamin Sylvia, Lester William A, Lowe Gillian C, Dutt Tina, Hill Quentin A, Scully Marie
Department of Haematology, University College London Hospital, London, United Kingdom.
Centre for Haemostasis and Thrombosis, St. Thomas' Hospital, London, United Kingdom.
Blood Adv. 2017 Jun 26;1(15):1159-1166. doi: 10.1182/bloodadvances.2017008268. eCollection 2017 Jun 27.
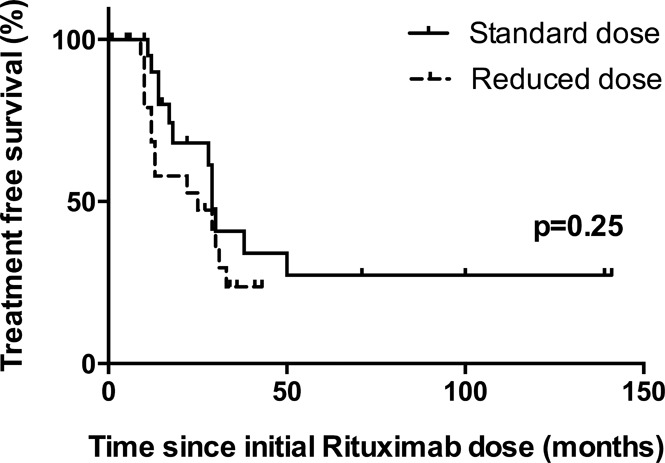
Acute antibody-mediated thrombotic thrombocytopenic purpura (TTP) is a thrombotic microangiopathy with high morbidity and mortality. Rituximab is highly effective as prophylaxis in patients at risk of acute TTP relapse, but the ideal dosing regimen is unknown. A multicenter retrospective cohort study evaluated outcomes of patients given rituximab prophylaxis to prevent TTP relapse. Rituximab was given in 76 episodes to 45 patients (34 women and 11 men). Four once-per-week infusions of standard- (375 mg/m [24 episodes]), reduced- (200 mg [19 episodes]), and intermediate- (500 mg [17 episodes]) dose rituximab were given; in the remaining 16 episodes, patients received 100 to 1000 mg rituximab in 1 to 5 doses. Patients were deemed at high risk of TTP relapse on the basis of ADAMTS13 activity dropping to ≤15% from the normal range. Preprophylaxis median ADAMTS13 level was 5% (range, <5% to 17%). Normalization of ADAMTS13 occurred in 78.9% of patients, with 92.1% having at least a partial response (ADAMTS13 ≥30%); 3 patients had no response. Over a median of 15 months (range, 1-141 months), there were only 3 TTP relapses (2 of these subacute) in the reduced dose group. Re-treatment with rituximab occurred in 50% of patient episodes at a median of 17.5 months (range, 9-112 months) after initial prophylaxis. There was a statistically higher rate of re-treatment in the reduced- vs standard-dose group: 0.38 vs 0.17 episodes per year, respectively. Treatment was generally well tolerated, infusional effects being the most commonly reported. Rituximab therapy is effective as prophylaxis for normalizing ADAMTS13 and is an additional measure for preventing acute TTP relapses in patients with immune TTP.
急性抗体介导的血栓性血小板减少性紫癜(TTP)是一种发病率和死亡率都很高的血栓性微血管病。利妥昔单抗对有急性TTP复发风险的患者进行预防非常有效,但理想的给药方案尚不清楚。一项多中心回顾性队列研究评估了接受利妥昔单抗预防以防止TTP复发的患者的结局。45例患者(34名女性和11名男性)共76次接受了利妥昔单抗治疗。分别给予4次每周一次的标准剂量(375mg/m[24次])、减量剂量(200mg[19次])和中等剂量(500mg[17次])的利妥昔单抗;在其余16次治疗中,患者接受1至5剂100至1000mg的利妥昔单抗。根据ADAMTS13活性从正常范围降至≤15%,判定患者有较高的TTP复发风险。预防前ADAMTS13水平中位数为5%(范围,<5%至17%)。78.9%的患者ADAMTS13恢复正常,92.1%的患者至少有部分反应(ADAMTS13≥30%);3例患者无反应。在中位15个月(范围,1 - 141个月)内,减量剂量组仅发生3次TTP复发(其中2次为亚急性)。50%的患者在初始预防后中位17.5个月(范围,9 - 112个月)进行了利妥昔单抗再治疗。减量剂量组与标准剂量组的再治疗率在统计学上有差异:分别为每年0.38次和0.17次。治疗一般耐受性良好,最常报告的是输液反应。利妥昔单抗治疗作为使ADAMTS13恢复正常的预防措施是有效的,并且是预防免疫性TTP患者急性TTP复发的一项额外措施。