de Vos Sven, Wagner-Johnston Nina D, Coutre Steven E, Flinn Ian W, Schreeder Marshall T, Fowler Nathan H, Sharman Jeff P, Boccia Ralph V, Barrientos Jacqueline C, Rai Kanti R, Boyd Thomas E, Furman Richard R, Kim Yeonhee, Godfrey Wayne R, Leonard John P
David Geffen School of Medicine at UCLA, Los Angeles, CA.
Washington University School of Medicine, St. Louis, MO.
Blood Adv. 2016 Nov 30;1(2):122-131. doi: 10.1182/bloodadvances.2016000976. eCollection 2016 Dec 13.
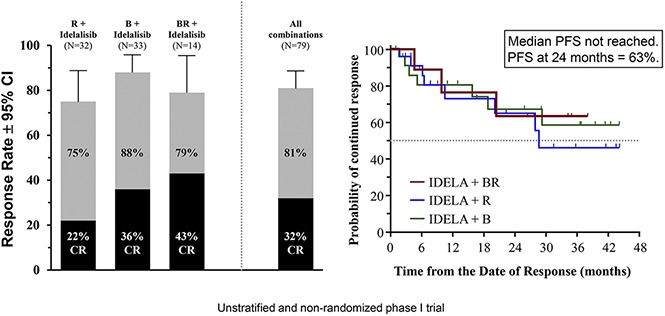
Idelalisib, a first-in-class oral inhibitor of phosphatidylinositol-3-kinase δ, has shown considerable antitumor activity as a monotherapy in recurrent indolent non-Hodgkin lymphoma (iNHL). To evaluate the safety and activity of idelalisib in combination with immunotherapy, chemotherapy, or both, 79 patients with relapsed/refractory iNHL were enrolled based on investigator preference in 3 treatment groups. Patients received continuous idelalisib in combination with (1) rituximab (IR; 375 mg/m weekly × 8 doses), (2) bendamustine (IB; 90 mg/m per day × 2, for 6 cycles), or (3) both bendamustine and rituximab at aforementioned doses (IBR; monthly × 6 cycles). Patients had a median age of 61 years, a median of 3 prior therapies, and 46% had refractory disease. The overall response rate was 75% (22% complete response) for IR, 88% (36%) for IB, and 79% (43%) for IBR. The median progression-free survival was 37.1 months overall: 29.7 months for IR, 32.8 for IB, and 37.1 months for IBR. The median duration of response was 28.6 months in the IR group and has not been reached in the IB and IBR groups. The most common grade ≥3 adverse events and laboratory abnormalities were neutropenia (41%), pneumonia (19%), transaminase elevations (16%), diarrhea/colitis (15%), and rash (9%). The safety and efficacy reflected in these early data, however, stand in contrast with later observations of significant toxicity in subsequent phase 3 trials in frontline chronic lymphocytic leukemia and less heavily pretreated iNHL patients. Our findings highlight the limitations of phase 1 trial data in the assessment of new regimens. This trial was registered at www.clinicaltrials.gov as #NCT01088048 (an extension study was registered at www.clinicaltrials.gov as #NCT01090414).
idelalisib是首个用于临床的磷脂酰肌醇-3-激酶δ口服抑制剂,作为单一疗法在复发性惰性非霍奇金淋巴瘤(iNHL)中显示出可观的抗肿瘤活性。为评估idelalisib联合免疫疗法、化疗或两者的安全性和活性,根据研究者的偏好,将79例复发/难治性iNHL患者纳入3个治疗组。患者接受持续的idelalisib联合(1)利妥昔单抗(IR;375mg/m²每周一次,共8剂),(2)苯达莫司汀(IB;90mg/m²每天一次,共2天,共6个周期),或(3)上述剂量的苯达莫司汀和利妥昔单抗(IBR;每月一次,共6个周期)。患者的中位年龄为61岁,既往治疗的中位次数为3次,46%的患者患有难治性疾病。IR组的总缓解率为75%(22%为完全缓解),IB组为88%(36%),IBR组为79%(43%)。总体中位无进展生存期为37.1个月:IR组为29.7个月,IB组为32.8个月,IBR组为37.1个月。IR组的中位缓解持续时间为28.6个月,IB组和IBR组尚未达到。最常见的≥3级不良事件和实验室异常为中性粒细胞减少(41%)、肺炎(19%)、转氨酶升高(16%)、腹泻/结肠炎(15%)和皮疹(9%)。然而,这些早期数据所反映的安全性和有效性与后来在一线慢性淋巴细胞白血病和预处理较轻的iNHL患者的后续3期试验中观察到的显著毒性形成对比。我们的研究结果突出了1期试验数据在评估新方案方面的局限性。本试验已在www.clinicaltrials.gov注册,编号为#NCT01088048(一项扩展研究已在www.clinicaltrials.gov注册,编号为#NCT01090414)。