Abdel-Hamid Ibrahim A, Ali Omar I
Division of Andrology, Mansoura Faculty of Medicine, Mansoura, Egypt.
Faculty of Medicine and Surgery, 6th October University, 6th October City, Egypt.
World J Mens Health. 2018 Jan;36(1):22-40. doi: 10.5534/wjmh.17051.
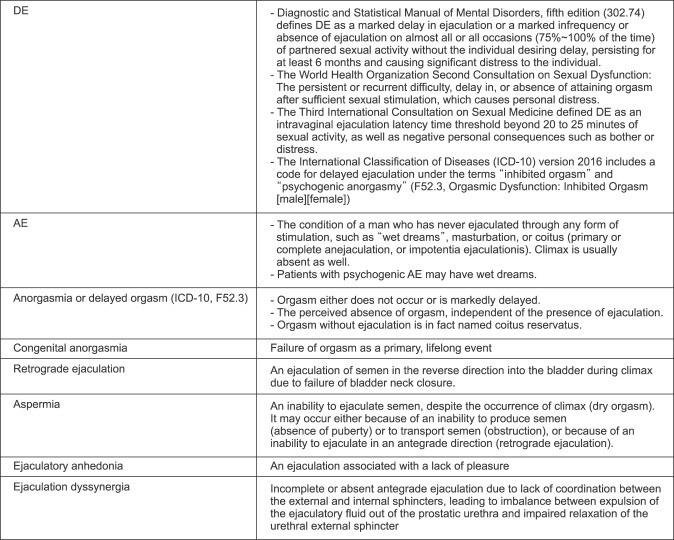
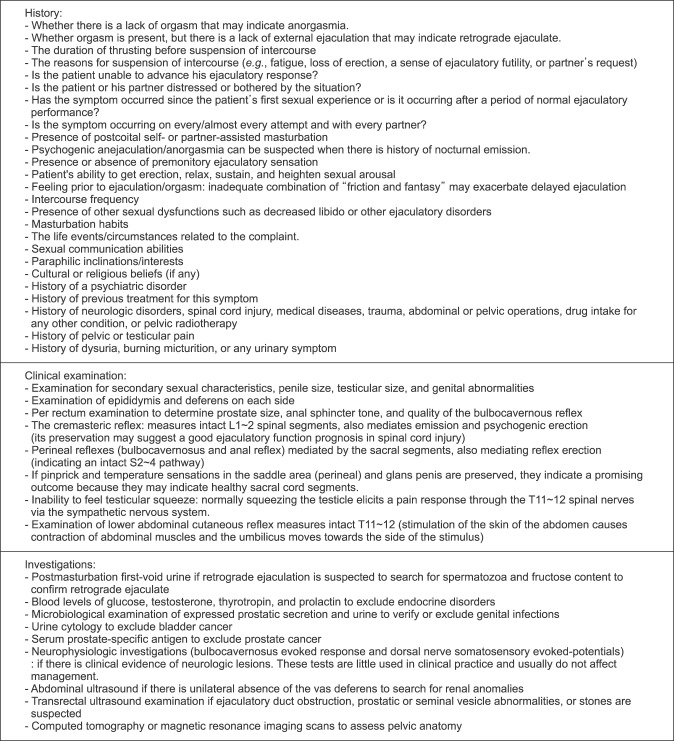
Delayed ejaculation (DE) is a poorly defined and uncommon form of male sexual dysfunction, characterized by a marked delay in ejaculation or an inability to achieve ejaculation. It is often quite concerning to patients and their partners, and sometimes frustrates couples' attempts to conceive. This article aims to review the pathophysiology of DE and anejaculation (AE), to explore our current understanding of the diagnosis, and to present the treatment options for this condition. Electronic databases were searched from 1966 to October 2017, including PubMed (MEDLINE) and Embase. We combined "delayed ejaculation," "retarded ejaculation," "inhibited ejaculation," or "anejaculation" as Medical Subject Headings (MeSH) terms or keywords with "epidemiology," "etiology," "pathophysiology," "clinical assessment," "diagnosis," or "treatment." Relevant sexual medicine textbooks were searched as well. The literature suggests that the pathophysiology of DE/AE is multifactorial, including both organic and psychosocial factors. Despite the many publications on this condition, the exact pathogenesis is not yet known. There is currently no single gold standard for diagnosing DE/AE, as operationalized criteria do not exist. The history is the key to the diagnosis. Treatment should be cause-specific. There are many approaches to treatment planning, including various psychological interventions, pharmacotherapy, and specific treatments for infertile men. An approved form of drug therapy does not exist. A number of approaches can be employed for infertile men, including the collection of nocturnal emissions, prostatic massage, prostatic urethra catheterization, penile vibratory stimulation, probe electroejaculation, sperm retrieval by aspiration from either the vas deferens or the epididymis, and testicular sperm extraction.
延迟射精(DE)是一种定义不明确且不常见的男性性功能障碍形式,其特征为射精明显延迟或无法射精。这常常令患者及其伴侣深感担忧,有时还会挫败夫妻受孕的努力。本文旨在综述延迟射精和无射精(AE)的病理生理学,探讨我们目前对其诊断的理解,并介绍针对这种情况的治疗选择。我们检索了1966年至2017年10月的电子数据库,包括PubMed(MEDLINE)和Embase。我们将“延迟射精”“射精迟缓”“射精抑制”或“无射精”作为医学主题词(MeSH)术语或关键词,与“流行病学”“病因学”“病理生理学”“临床评估”“诊断”或“治疗”相结合进行检索。同时也检索了相关的性医学教科书。文献表明,延迟射精/无射精的病理生理学是多因素的,包括器质性和心理社会因素。尽管关于这种情况有许多出版物,但确切的发病机制尚不清楚。目前尚无诊断延迟射精/无射精的单一金标准,因为尚未存在可操作的标准。病史是诊断的关键。治疗应针对病因。治疗方案有很多种,包括各种心理干预、药物治疗以及针对不育男性的特定治疗。目前不存在已获批的药物治疗形式。对于不育男性可以采用多种方法,包括收集夜间遗精、前列腺按摩、前列腺尿道插管、阴茎振动刺激、探针电射精、经输精管或附睾抽吸取精以及睾丸精子提取。