Perelman Michael A
Human Sexuality Program, NY Weill Cornell Medical Center, New York, USA.
Transl Androl Urol. 2016 Aug;5(4):563-75. doi: 10.21037/tau.2016.07.05.
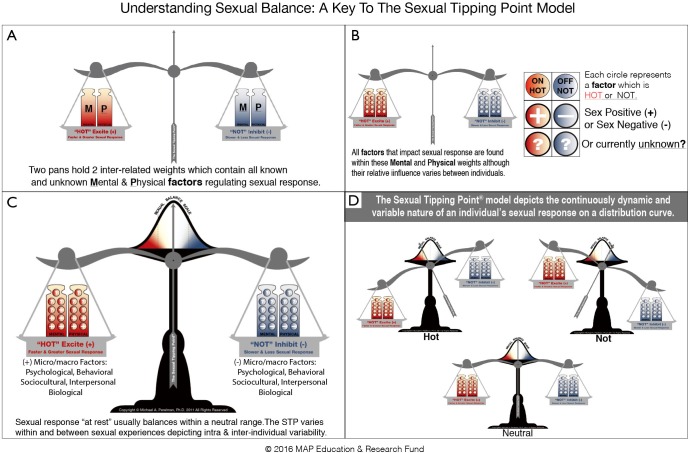
The Sexual Tipping Point(®) (STP) model is an integrated approach to the etiology, diagnosis and treatment of men with delayed ejaculation (DE), including all subtypes manifesting ejaculatory delay or absence [registered trademark owned by the MAP Educational Fund, a 501(c)(3) public charity]. A single pathogenetic pathway does not exist for sexual disorders generally and that is also true for DE specifically. Men with DE have various bio-psychosocial-behavioral & cultural predisposing, precipitating, maintaining, and contextual factors which trigger, reinforce, or worsen the probability of DE occurring. Regardless of the degree of organic etiology present, DE is exacerbated by insufficient stimulation: an inadequate combination of "friction and fantasy". High frequency negative thoughts may neutralize erotic cognitions (fantasy) and subsequently delay, ameliorate, or inhibit ejaculation, while partner stimulation (friction) may prove unsatisfying. Assessment requires a thorough sexual history including inquiry into masturbatory methods. Many men with DE engage in an idiosyncratic masturbatory style, defined as a masturbation technique not easily duplicated by the partner's hand, mouth, or vagina. The clinician's most valuable diagnostic tool is a focused sex history (sex status). Differentiate DE from other sexual problems and review the conditions under which the man can ejaculate. Perceived partner attractiveness, the use of fantasy during sex, anxiety-surrounding coitus and masturbatory patterns require meticulous exploration. Identify important DE causes by juxtaposing an awareness of his cognitions and the sexual stimulation experienced during masturbation, versus a partnered experience. Assist the man in identifying behaviors that enhance immersion in excitation and minimize inhibiting thoughts, in order to reach ejaculation in his preferred manner. Discontinuing, reducing or altering masturbation is often required, which evokes patient resistance. Coaching tips are offered on how to ensure adherence to this suspension, manage resistance and facilitate success. Depending on motivation level, masturbation interruption may be compromised and negotiated. Encourage a man who continues to masturbate to alter style ("switch hands") and to approximate the stimulation likely to be experienced with his partner. Success will require most men to be taught to learn bodily movements and fantasies that approximate the thoughts and sensations experienced in masturbation. Fertility issues, as well as patient/partner anger are important causational factors, which often require individual and/or conjoint consultation. Drug treatment would benefit men particularly with severe DE, regardless of concomitant psychosocial-behavioral and cultural complications. When and if a safe effective medication for DE becomes available, this author's transdisciplinary perspective supports appropriate medication use when integrated with counseling. This approach emphasizes the utility of a biopsychosocial-cultural perspective combined with special attention to the patient's narrative. Treatment is patient-centered, holistic and integrates a variety of therapies as needed.
性临界点(®)(STP)模型是一种针对射精延迟(DE)男性的病因、诊断和治疗的综合方法,包括表现为射精延迟或缺失的所有亚型[由MAP教育基金(一家501(c)(3)公共慈善机构)拥有的注册商标]。一般来说,性功能障碍不存在单一的致病途径,射精延迟(DE)尤其如此。患有射精延迟(DE)的男性具有各种生物心理社会行为和文化方面的易感、促发、维持和情境因素,这些因素会引发、强化或增加射精延迟(DE)发生的可能性。无论存在何种程度的器质性病因,刺激不足都会加剧射精延迟(DE):即“摩擦和幻想”的不充分结合。高频消极思维可能会抵消性幻想认知,进而延迟、改善或抑制射精,而伴侣的刺激(摩擦)可能并不令人满意。评估需要全面的性史,包括询问手淫方式。许多患有射精延迟(DE)的男性采用独特的手淫方式,即一种伴侣的手、口或阴道不易复制的手淫技巧。临床医生最有价值的诊断工具是详细的性史(性状况)。将射精延迟(DE)与其他性问题区分开来,并了解该男性能够射精的条件。伴侣的吸引力感知、性行为中幻想的使用、性交时的焦虑以及手淫模式都需要仔细探究。通过对比他的认知以及手淫时的性刺激与性伴侣体验,找出射精延迟(DE)的重要原因。帮助该男性识别能够增强兴奋沉浸感并减少抑制性思维的行为,以便以他喜欢的方式射精。通常需要停止、减少或改变手淫方式,这往往会引起患者的抵触情绪。文中提供了指导建议,说明如何确保坚持这种暂停手淫的做法、应对抵触情绪并促进成功。根据动机水平,手淫中断可能需要妥协和协商。鼓励继续手淫的男性改变方式(“换只手”),并模拟可能在与性伴侣性行为时体验到的刺激。大多数男性需要学习身体动作和幻想,以近似手淫时的思维和感觉,才能取得成功。生育问题以及患者/伴侣的愤怒是重要的致病因素,通常需要进行个体和/或联合咨询。药物治疗对患有严重射精延迟(DE)的男性有益,无论是否伴有心理社会行为和文化方面的并发症。当且如果有一种安全有效的治疗射精延迟(DE)的药物可用时,本文作者的跨学科观点支持在结合咨询的情况下合理使用药物。这种方法强调生物心理社会文化视角的实用性,并特别关注患者的叙述。治疗以患者为中心,全面且根据需要整合多种疗法。