Magazine Rahul, Surendra Vyshak Uddur, Chogtu Bharti
Department of Pulmonary Medicine, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
Department of Pharmacology, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
Lung India. 2018 Jan-Feb;35(1):16-20. doi: 10.4103/lungindia.lungindia_226_17.
The need for more effective management of acute asthma has led to research on drugs which are otherwise approved for use in chronic asthma.
To study and compare the effects of oral montelukast with oral ozagrel in acute asthma.
One hundred and twenty patients with acute asthma were recruited for the study. Out of 120 study patients, forty each were randomized into placebo, montelukast, and ozagrel groups. After the first dose of the drug or placebo was administered, peak expiratory flow rate (PEFR), number of rescue medications and also vital signs were noted at 6 h, 12 h, 24 h, 48 h, and at discharge. In addition, same recordings were done on the morning (8 a.m. - 10 a.m.) following admission. The difference in mean PEFR of each group at above-mentioned time points was the primary endpoint whereas need for rescue medications the secondary end-point.
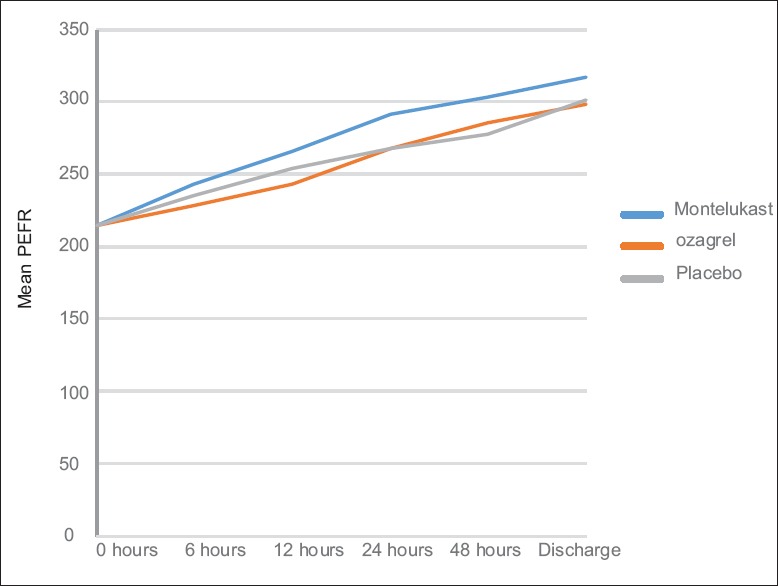
The respective mean PEFR recordings of the placebo, montelukast, and ozagrel groups at various time points were as follows: at 6 h (235.19 ± 3.18, 242.86 ± 3.26, 228.18 ± 3.25); at 12 h (254.37 ± 5.23, 265.62 ± 5.38, 242.99 ± 5.36); at 24 h (267.46 ± 7.41, 291.39 ± 7.61, 268.14 ± 7.58); and at 48 h (277.99 ± 7.35, 303.22 ± 7.56, 285.27 ± 7.53); and discharge (301.94 ± 7.07, 317.32 ± 7.27, 298.99 ± 7.23). The mean PEFR between the treatment groups were not statistically significant (P = 0.102). The mean PEFR in the three groups at 8-10 a.m. following admission was 257.60 ± 5.52, 264.23 ± 5.98, and 249.94 ± 5.96; P = 0.266. Total number of rescue doses needed were 7, 4, and 13, respectively (P = 0.67).
Montelukast or ozagrel when added to the standard treatment of acute asthma does not result in any additional benefit.
对急性哮喘进行更有效管理的需求促使人们对原本已获批用于慢性哮喘的药物展开研究。
研究并比较口服孟鲁司特与口服奥扎格雷对急性哮喘的疗效。
招募120例急性哮喘患者进行本研究。在120例研究患者中,每组40例,分别随机分为安慰剂组、孟鲁司特组和奥扎格雷组。在给予首剂药物或安慰剂后,于6小时、12小时、24小时、48小时及出院时记录呼气峰值流速(PEFR)、急救药物使用次数以及生命体征。此外,在入院后的次日上午(上午8点至10点)进行相同记录。各治疗组在上述时间点的平均PEFR差异为主要终点,而急救药物的使用需求为次要终点。
安慰剂组、孟鲁司特组和奥扎格雷组在各时间点的平均PEFR记录如下:6小时(235.19±3.18、242.86±3.26、228.18±3.25);12小时(254.37±5.23、265.62±5.38、242.99±5.36);24小时(267.46±7.41、291.39±7.61、268.14±7.58);48小时(277.99±7.35、303.22±7.56、285.27±7.53);出院时(301.94±7.07、317.32±7.27、298.99±7.23)。各治疗组之间的平均PEFR差异无统计学意义(P = 0.102)。入院次日上午8点至10点时,三组的平均PEFR分别为257.60±5.52、264.23±5.98和249.94±5.96;P = 0.266。所需急救剂量总数分别为7次、4次和13次(P = 0.67)。
在急性哮喘标准治疗基础上加用孟鲁司特或奥扎格雷未带来任何额外益处。