Niu Xiaowei, Zhang Jingjing, Bai Ming, Peng Yu, Sun Shaobo, Zhang Zheng
The First School of Clinical Medicine, Lanzhou University, Tianshui South Road, No. 222, Lanzhou, Gansu, 730000, China.
Baiyin Second People's Hospital, Gongyuan Road, No. 509, Baiyin, Gansu, 730900, China.
BMC Cardiovasc Disord. 2018 Jan 10;18(1):3. doi: 10.1186/s12872-017-0722-z.
Despite the restoration of epicardial flow after primary percutaneous coronary intervention (PPCI), myocardial reperfusion remains impaired in a significant proportion of patients. We performed a network meta-analysis to assess the effect of 7 intracoronary agents (adenosine, anisodamine, diltiazem, nicorandil, nitroprusside, urapidil, and verapamil) on the no-reflow phenomenon in patients with ST-elevation myocardial infarction (STEMI) undergoing PPCI.
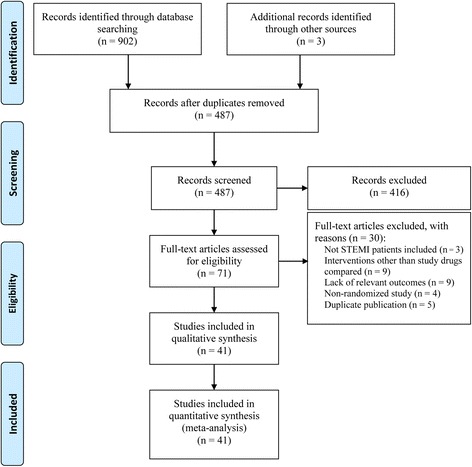
Database searches were conducted to identify randomized controlled trials (RCTs) comparing the 7 agents with each other or with standard PPCI. Outcome measures included thrombolysis in myocardial infarction flow grade (TFG), ST-segment resolution (STR), left ventricular ejection fraction (LVEF), major adverse cardiovascular events (MACEs), and adverse events.
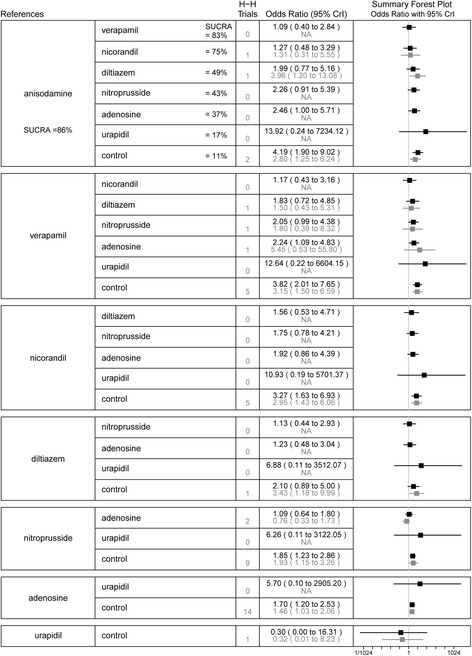
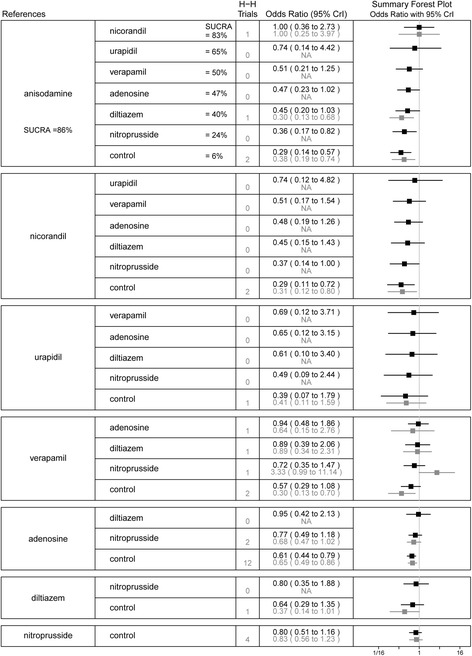
Forty-one RCTs involving 4069 patients were analyzed. The addition of anisodamine to standard PPCI for STEMI was associated with improved post-procedural TFG, more occurrences of STR, and improvement of LVEF. The cardioprotective effect of anisodamine conferred a MACE-free survival benefit. Additionally, nitroprusside was regarded as efficient in improving coronary flow and clinical outcomes. Compared with standard care, adenosine, nicorandil, and verapamil improved coronary flow but had no corresponding benefits regarding cardiac function and clinical outcomes. The ranking probability for the 7 treatment drugs showed that anisodamine consistently ranked the highest in efficacy outcomes (TFG < 3, STR, LVEF, and MACEs). No severe adverse events, such as hypotension and malignant arrhythmia, were observed in patients treated with anisodamine. Network meta-regression analysis showed that age, the time to reperfusion, and study follow-up did not affect the treatment effects.
The intracoronary administration of anisodamine appears to improve myocardial reperfusion, cardiac function, and clinical outcomes in patients with STEMI undergoing PPCI. Given the limited quality and quantity of the included studies, more rigorous RCTs are needed to verify the role of this inexpensive and well-tolerated regimen.
尽管在直接经皮冠状动脉介入治疗(PPCI)后心外膜血流得以恢复,但仍有相当一部分患者的心肌再灌注受损。我们进行了一项网状Meta分析,以评估7种冠状动脉内用药(腺苷、山莨菪碱、地尔硫䓬、尼可地尔、硝普钠、乌拉地尔和维拉帕米)对接受PPCI的ST段抬高型心肌梗死(STEMI)患者无复流现象的影响。
进行数据库检索,以识别将这7种药物相互比较或与标准PPCI比较的随机对照试验(RCT)。结局指标包括心肌梗死溶栓血流分级(TFG)、ST段回落(STR)、左心室射血分数(LVEF)、主要不良心血管事件(MACE)和不良事件。
分析了涉及4069例患者的41项RCT。在STEMI的标准PPCI中加用山莨菪碱与术后TFG改善、STR发生率增加和LVEF改善相关。山莨菪碱的心脏保护作用带来了无MACE生存获益。此外,硝普钠被认为在改善冠状动脉血流和临床结局方面有效。与标准治疗相比,腺苷、尼可地尔和维拉帕米改善了冠状动脉血流,但在心脏功能和临床结局方面没有相应益处。这7种治疗药物的排序概率显示,山莨菪碱在疗效结局(TFG<3、STR、LVEF和MACE)方面始终排名最高。在接受山莨菪碱治疗的患者中未观察到严重不良事件,如低血压和恶性心律失常。网状Meta回归分析显示,年龄、再灌注时间和研究随访不影响治疗效果。
冠状动脉内给予山莨菪碱似乎可改善接受PPCI的STEMI患者的心肌再灌注、心脏功能和临床结局。鉴于纳入研究的质量和数量有限,需要更严格的RCT来验证这种廉价且耐受性良好的治疗方案的作用。