Department of Obstetrics and Gynaecology, Lagos State University College of Medicine/Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria.
BMC Pregnancy Childbirth. 2018 Jan 10;18(1):24. doi: 10.1186/s12884-017-1643-7.
Caesarean delivery carries a risk of major intra-operative blood loss and its performance is often delayed by non-availability of blood and blood products. Unnecessary cross-matching and reservation of blood lead to apparent scarcity in centres with limited supply. This study set out to identify the risk factors for blood transfusion in women who underwent caesarean delivery at a tertiary obstetric unit with a view to ensuring efficient blood utilization.
A prospective cohort analysis of 906 women who had caesarean deliveries at the Lagos State University Teaching Hospital, Nigeria between January and December, 2011. A comparison was made between 188 women who underwent blood transfusion and 718 who did not. Data were obtained on a daily basis by investigators from patients, clinical notes and referral letters using structured pre-tested data collecting form. Socio-demographic characteristics; antenatal, perioperative and intraoperative details; blood loss; transfusion; and puerperal observations were recorded. EPI-Info statistical software version 3.5.3 was used for multivariable analysis to determine independent risk factors for blood transfusion.
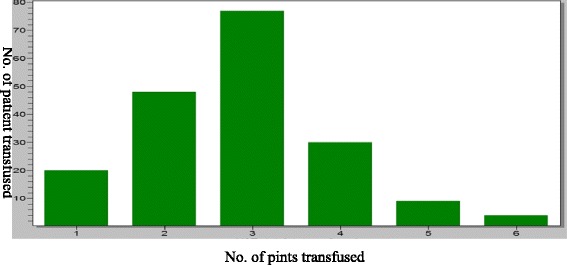
Of the 2134 deliveries during the study period, 906 (42.5%) had caesarean deliveries and of which 188 (20.8%) were transfused. The modal unit of blood transfused was 3 pints (41.3%). The most common indication for caesarean section was cephalo-pelvic disproportion (25.7%).The independent risk factors for blood transfusion at caesarean section were second stage Caesarean Section (aOR = 76.14, 95% CI = 1.25-4622.06, p = 0.04), placenta previa (aOR = 32.57, 95% CI = 2.22-476.26, p = 0.01), placental abruption (aOR = 25.35, 95% CI = 3.06-211.02, p < 0.001), pre-operative anaemia (aOR = 12.15, 95% = CI 4.02-36.71, p < 0.001), prolonged operation time (aOR = 10.72 95% CI = 1.37-36.02, p < 0.001), co-morbidities like previous uterine scar (aOR = 7.02, 95% CI = 1.37-36.02, p = 0.02) and hypertensive disorders in pregnancy (aOR = 5.19, 95% CI = 1.84-14.68, p < 0.001). Obesity reduced the risk for blood transfusion (aOR = 0.24, 95% CI = 0.09-0.61, p = 0.0024).
The overall risk of blood transfusion in cesarean delivery is high. Paturients with the second stage Caesarean section, placenta previa, abruptio placentae and preoperative maternal anaemia have an increased risk of blood transfusion. Hence, adequate peri-operative preparations for blood transfusion are essential in these situations. Optimizing maternal hemoglobin concentration during antenatal period may reduce the incidence of caesarean-associated blood transfusion.
剖宫产术中存在大量术中失血的风险,由于血液和血液制品的供应不足,其实施经常会延迟。不必要的交叉配型和血液储备会导致供应有限的中心明显出现血液短缺。本研究旨在确定在尼日利亚拉各斯州立大学教学医院行剖宫产术的妇女输血的风险因素,以期确保血液的有效利用。
对 2011 年 1 月至 12 月期间在尼日利亚拉各斯州立大学教学医院行剖宫产术的 906 名妇女进行前瞻性队列分析。比较了 188 名输血妇女和 718 名未输血妇女。研究人员每天从患者、临床记录和转诊信中获取数据,使用经过预测试的结构化数据收集表。记录了社会人口统计学特征;产前、围手术期和手术期间的详细信息;失血量;输血;和产褥期观察。使用 EPI-Info 统计软件版本 3.5.3 进行多变量分析,以确定输血的独立风险因素。
在研究期间的 2134 次分娩中,906 次(42.5%)行剖宫产术,其中 188 次(20.8%)输血。输血的平均单位为 3 品脱(41.3%)。剖宫产最常见的指征是头盆不称(25.7%)。剖宫产术输血的独立风险因素包括第二产程剖宫产(aOR=76.14,95%CI=1.25-4622.06,p=0.04)、前置胎盘(aOR=32.57,95%CI=2.22-476.26,p=0.01)、胎盘早剥(aOR=25.35,95%CI=3.06-211.02,p<0.001)、术前贫血(aOR=12.15,95%CI=4.02-36.71,p<0.001)、手术时间延长(aOR=10.72 95%CI=1.37-36.02,p<0.001)、既往子宫瘢痕等合并症(aOR=7.02,95%CI=1.37-36.02,p=0.02)和妊娠高血压疾病(aOR=5.19,95%CI=1.84-14.68,p<0.001)。肥胖降低了输血的风险(aOR=0.24,95%CI=0.09-0.61,p=0.0024)。
剖宫产术中输血的总体风险很高。第二产程剖宫产、前置胎盘、胎盘早剥和术前母体贫血的患者有输血的风险增加。因此,在这些情况下,应充分做好围手术期输血准备。在产前期间优化母体血红蛋白浓度可能会降低与剖宫产相关的输血发生率。