Conway Baqiyyah N, Han Xijing, Munro Heather M, Gross Amy L, Shu Xiao-Ou, Hargreaves Margaret K, Zheng Wei, Powers Alvin C, Blot William J
Department of Epidemiology and Biostatistics, University of Texas Health Science Center, Tyler, Texas, United States of America.
International Epidemiology Field Station, Vanderbilt Institute for Clinical and Translational Research, Vanderbilt University Medical Center, Rockville, Maryland, United States of America.
PLoS One. 2018 Jan 11;13(1):e0190993. doi: 10.1371/journal.pone.0190993. eCollection 2018.
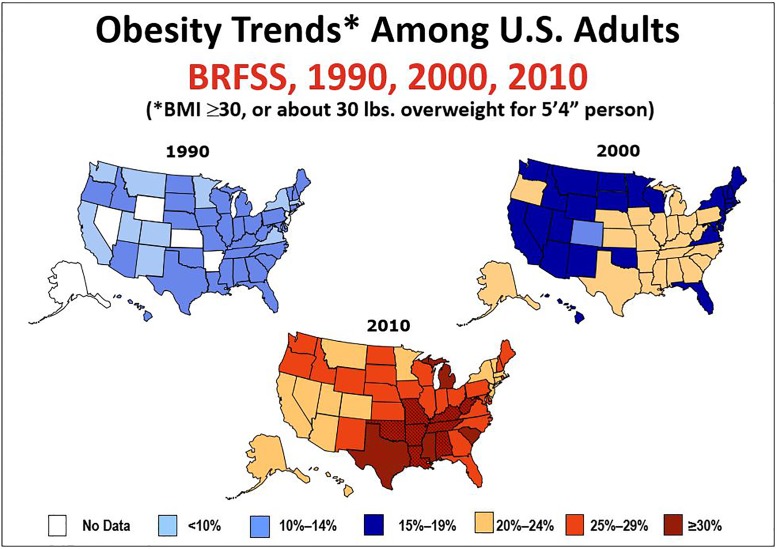
Obesity is known to be a major risk factor for diabetes, but the magnitude of risk and variation between blacks and whites are less well documented in populations heavily affected by obesity. Herein we assess rates and risks of incident diabetes in a diverse southern population where obesity is common.
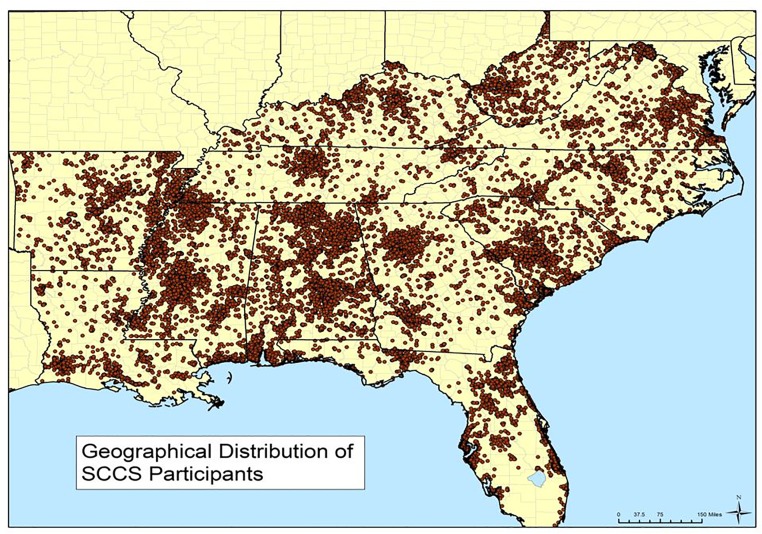
A total of 24,000 black and 14,064 white adults aged 40-79 in the Southern Community Cohort Study with no self-reported diabetes at study enrollment during 2002-2009 was followed for up to 10 (median 4.5) years. Incidence rates, odds ratios (OR) and accompanying 95% confidence intervals (CI) for medication-treated incident diabetes were determined according to body mass index (BMI) and other characteristics, including tobacco and alcohol consumption, healthy eating and physical activity indices, and socioeconomic status (SES).
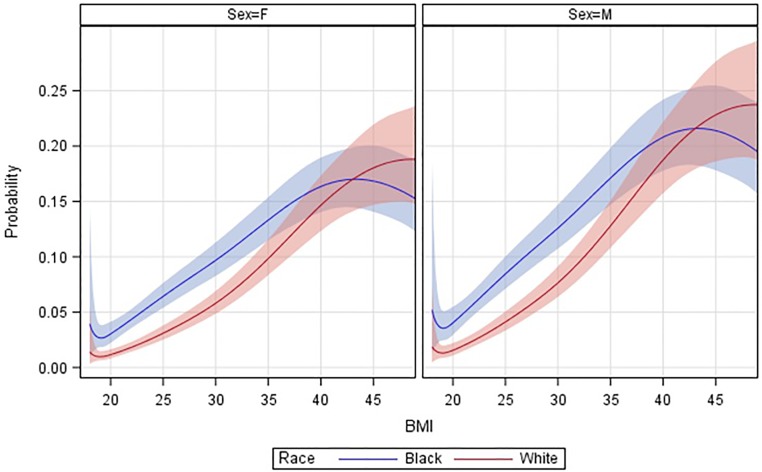
Risk of incident diabetes rose monotonically with increasing BMI, but the trends differed between blacks and whites (pinteraction < .0001). Adjusted ORs (CIs) for diabetes among those with BMI≥40 vs 20-25 kg/m2 were 11.9 (8.4-16.8) for whites and 4.0 (3.3-4.8) for blacks. Diabetes incidence was more than twice as high among blacks than whites of normal BMI, but the racial difference became attenuated as BMI rose, with estimated 5-year probabilities of developing diabetes approaching 20% for both blacks and whites with BMI≥40 kg/m2. Diabetes risk was also associated with low SES, significantly (pinteraction≤.02) more so for whites, current cigarette smoking, and lower healthy eating and physical activity indices, although high BMI remained the predominant risk factor among both blacks and whites. From baseline prevalence and 20-year projections of the incidence trends, we estimate that the large majority of surviving cohort participants with BMI≥40 kg/m2 will be diagnosed with diabetes.
Even using conservative criteria to ascertain diabetes incidence (i.e., requiring diabetes medication use and ignoring undiagnosed cases), rates of obesity-associated diabetes were exceptionally high in this low-income adult population. The findings indicate that effective strategies to halt the rising prevalence of obesity are needed to avoid substantial increases in diabetes in coming years.
肥胖是已知的糖尿病主要危险因素,但在受肥胖严重影响的人群中,黑人和白人之间的风险程度及差异尚无充分记录。在此,我们评估了肥胖常见的美国南部不同人群中糖尿病的发病率及风险。
南部社区队列研究中共有24,000名黑人及14,064名40 - 79岁的白人成年人,他们在2002 - 2009年研究入组时均无自我报告的糖尿病史,随访长达10年(中位数4.5年)。根据体重指数(BMI)及其他特征,包括烟草和酒精消费、健康饮食及身体活动指数以及社会经济地位(SES),确定药物治疗的新发糖尿病的发病率、比值比(OR)及相应的95%置信区间(CI)。
新发糖尿病的风险随BMI升高呈单调上升趋势,但黑人和白人的趋势有所不同(交互作用p <.0001)。BMI≥40 vs 20 - 25 kg/m²者中,白人糖尿病的校正OR(CI)为11.9(8.4 - 16.8),黑人为4.0(3.3 - 4.8)。正常BMI的黑人中糖尿病发病率是白人的两倍多,但随着BMI升高,种族差异逐渐减弱,BMI≥40 kg/m²的黑人和白人发生糖尿病的估计5年概率均接近20%。糖尿病风险还与低SES相关,白人中这种相关性更显著(交互作用p≤.02),与当前吸烟以及较低的健康饮食和身体活动指数也相关,尽管高BMI仍是黑人和白人中的主要危险因素。根据基线患病率及发病率趋势的20年预测,我们估计BMI≥40 kg/m²的队列存活参与者中,绝大多数将被诊断为糖尿病。
即使采用保守标准确定糖尿病发病率(即要求使用糖尿病药物治疗且忽略未确诊病例),在这个低收入成年人群中,肥胖相关糖尿病的发病率仍异常高。研究结果表明,需要采取有效的策略来阻止肥胖患病率的上升,以避免未来几年糖尿病大幅增加。