Kidney Research Institute, Harborview Medical Center, Division of Nephrology, University of Washington, Seattle, Washington.
Harold Simmons Center for Kidney Disease Research and Epidemiology, Division of Nephrology and Hypertension, University of California Irvine Medical Center, Irvine, California; and.
Clin J Am Soc Nephrol. 2018 Mar 7;13(3):445-455. doi: 10.2215/CJN.05680517. Epub 2018 Jan 11.
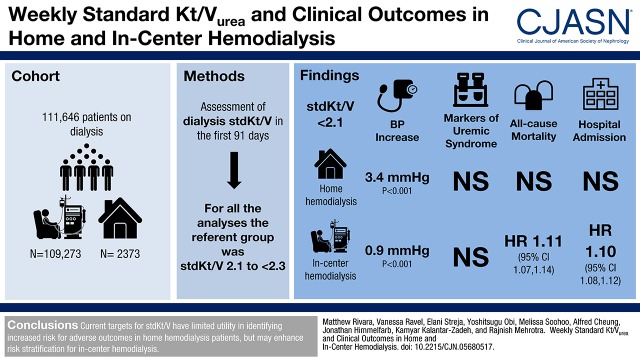
Patients undergoing hemodialysis with a frequency other than thrice weekly are not included in current clinical performance metrics for dialysis adequacy. The weekly standard Kt/V incorporates treatment frequency, but there are limited data on its association with clinical outcomes.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We used multivariable regression to examine the association of dialysis standard Kt/V with BP and metabolic control (serum potassium, calcium, bicarbonate, and phosphorus) in patients incidental to dialysis treated with home (=2373) or in-center hemodialysis (=109,273). We further used Cox survival models to examine the association of dialysis standard Kt/V with mortality, hospitalization, and among patients on home hemodialysis, transfer to in-center hemodialysis.
After adjustment for potential confounders, patients with dialysis standard Kt/V <2.1 had higher BPs compared with patients with standard Kt/V 2.1 to <2.3 (3.4 mm Hg higher [<0.001] for home hemodialysis and 0.9 mm Hg higher [<0.001] for in-center hemodialysis). There were no clinically meaningful associations between dialysis standard Kt/V and markers of metabolic control, irrespective of dialysis modality. There was no association between dialysis standard Kt/V and risk for mortality, hospitalization, or transfer to in-center hemodialysis among patients undergoing home hemodialysis. Among patients on in-center hemodialysis, dialysis standard Kt/V <2.1 was associated with higher risk (adjusted hazard ratio, 1.11; 95% confidence interval, 1.07 to 1.14) and standard Kt/V ≥2.3 was associated with lower risk (adjusted hazard ratio, 0.97; 95% confidence interval, 0.94 to 0.99) for death compared with standard Kt/V 2.1 to <2.3. Additional analyses limited to patients with available data on residual kidney function showed similar relationships of dialysis and total (dialysis plus kidney) standard Kt/V with outcomes.
Current targets for standard Kt/V have limited utility in identifying individuals at increased risk for adverse clinical outcomes for those undergoing home hemodialysis but may enhance risk stratification for in-center hemodialysis.
目前的透析充分性临床评估指标并不包括每周接受非三次透析治疗的患者。每周标准 Kt/V 纳入了治疗频率,但关于其与临床结局的相关性的数据有限。
设计、地点、参与者和测量:我们使用多变量回归分析,检查了透析标准 Kt/V 与血压和代谢控制(血清钾、钙、碳酸氢盐和磷)之间的相关性,这些患者是接受家庭(=2373)或中心血液透析(=109273)治疗的偶然患者。我们还使用 Cox 生存模型检查了透析标准 Kt/V 与死亡率、住院率的关系,以及在接受家庭血液透析的患者中,与转至中心血液透析的关系。
在调整了潜在混杂因素后,透析标准 Kt/V<2.1 的患者的血压高于透析标准 Kt/V 为 2.1 至<2.3 的患者(家庭血液透析高 3.4 毫米汞柱[<0.001],中心血液透析高 0.9 毫米汞柱[<0.001])。无论透析方式如何,透析标准 Kt/V 与代谢控制标志物之间均无临床意义上的关联。在接受家庭血液透析的患者中,透析标准 Kt/V 与死亡率、住院率或转至中心血液透析率之间无关联。在接受中心血液透析的患者中,透析标准 Kt/V<2.1 与较高的死亡风险相关(调整后的危险比,1.11;95%置信区间,1.07 至 1.14),而透析标准 Kt/V≥2.3 与较低的死亡风险相关(调整后的危险比,0.97;95%置信区间,0.94 至 0.99),与透析标准 Kt/V 为 2.1 至<2.3 相比。对有残余肾功能数据的患者进行的进一步分析表明,透析和总(透析加肾脏)标准 Kt/V 与结局的关系相似。
目前的标准 Kt/V 目标对于识别接受家庭血液透析的患者发生不良临床结局的风险增加的个体的作用有限,但可能增强对中心血液透析患者的风险分层。