Department of Medicine (Medical Oncology), Yale School of Medicine, Yale University, New Haven, Connecticut.
Department of Therapeutic Radiology, Yale School of Medicine, Yale University, New Haven, Connecticut.
Clin Cancer Res. 2018 Apr 15;24(8):1872-1880. doi: 10.1158/1078-0432.CCR-17-1341. Epub 2018 Jan 12.
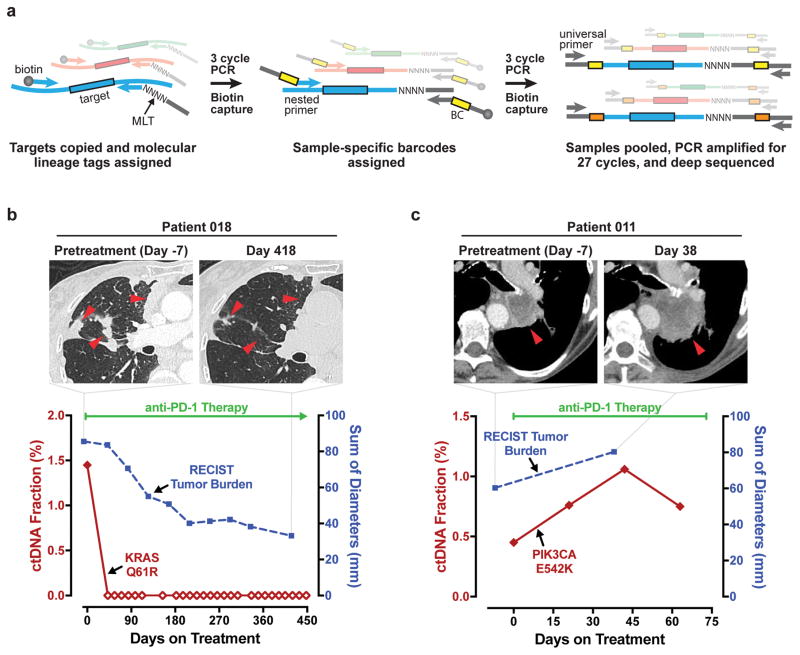
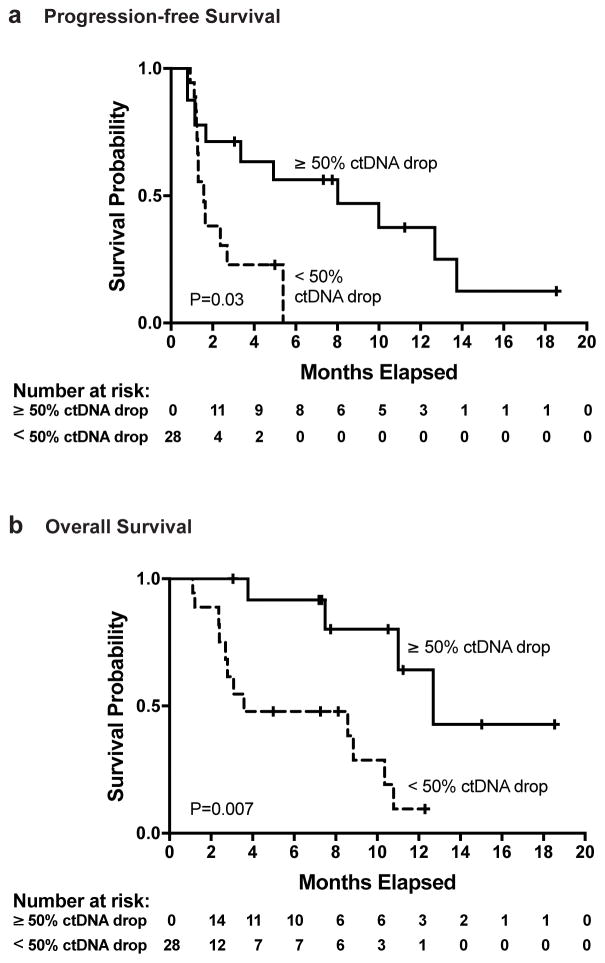
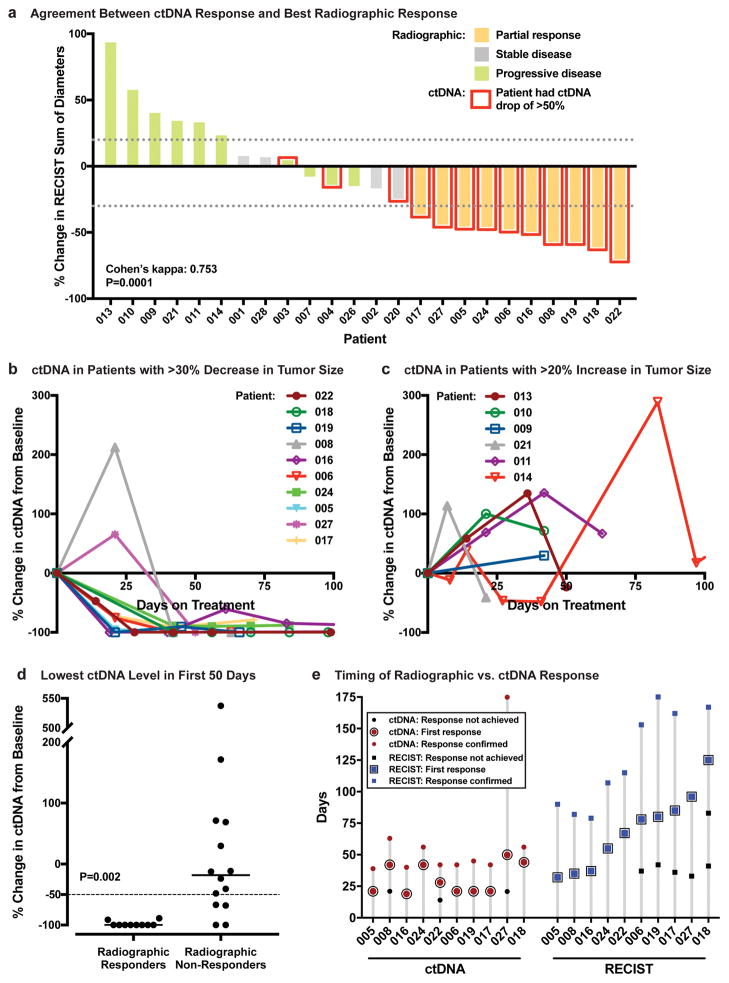
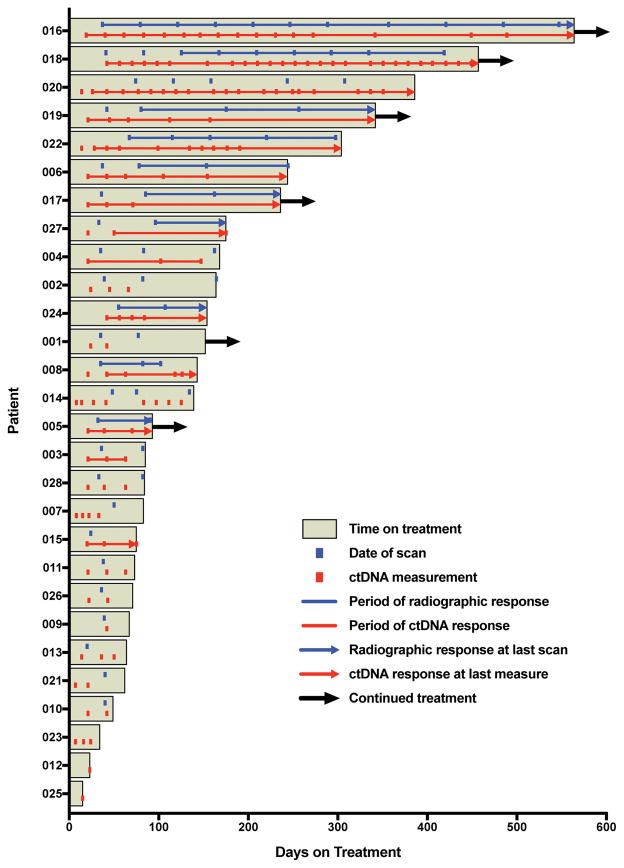
Decisions to continue or suspend therapy with immune checkpoint inhibitors are commonly guided by tumor dynamics seen on serial imaging. However, immunotherapy responses are uniquely challenging to interpret because tumors often shrink slowly or can appear transiently enlarged due to inflammation. We hypothesized that monitoring tumor cell death in real time by quantifying changes in circulating tumor DNA (ctDNA) levels could enable early assessment of immunotherapy efficacy. We compared longitudinal changes in ctDNA levels with changes in radiographic tumor size and with survival outcomes in 28 patients with metastatic non-small cell lung cancer (NSCLC) receiving immune checkpoint inhibitor therapy. CtDNA was quantified by determining the allele fraction of cancer-associated somatic mutations in plasma using a multigene next-generation sequencing assay. We defined a ctDNA response as a >50% decrease in mutant allele fraction from baseline, with a second confirmatory measurement. Strong agreement was observed between ctDNA response and radiographic response (Cohen's kappa, 0.753). Median time to initial response among patients who achieved responses in both categories was 24.5 days by ctDNA versus 72.5 days by imaging. Time on treatment was significantly longer for ctDNA responders versus nonresponders (median, 205.5 vs. 69 days; < 0.001). A ctDNA response was associated with superior progression-free survival [hazard ratio (HR), 0.29; 95% CI, 0.09-0.89; = 0.03], and superior overall survival (HR, 0.17; 95% CI, 0.05-0.62; = 0.007). A drop in ctDNA level is an early marker of therapeutic efficacy and predicts prolonged survival in patients treated with immune checkpoint inhibitors for NSCLC. .
我们假设,通过定量检测循环肿瘤 DNA(ctDNA)水平的变化来实时监测肿瘤细胞死亡,可能有助于早期评估免疫治疗的疗效。我们比较了 28 例接受免疫检查点抑制剂治疗的转移性非小细胞肺癌(NSCLC)患者的 ctDNA 水平的纵向变化与影像学肿瘤大小变化和生存结局。ctDNA 通过使用多基因下一代测序检测血浆中与癌症相关的体细胞突变的等位基因分数来定量。我们将 ctDNA 反应定义为基线时突变等位基因分数下降超过 50%,并进行第二次确认测量。ctDNA 反应与影像学反应之间观察到强烈的一致性(Cohen's kappa,0.753)。在两种类别中均达到反应的患者中,ctDNA 检测到的首次反应时间中位数为 24.5 天,而影像学检测到的为 72.5 天。ctDNA 反应者的治疗时间明显长于无反应者(中位数分别为 205.5 天和 69 天; < 0.001)。ctDNA 反应与无进展生存期的改善相关[风险比(HR),0.29;95%置信区间,0.09-0.89; = 0.03],总生存期也有改善[HR,0.17;95%置信区间,0.05-0.62; = 0.007]。ctDNA 水平的下降是治疗疗效的早期标志物,并预测接受免疫检查点抑制剂治疗的 NSCLC 患者的生存时间延长。.