Wang Tongtong, McNeill Ann Marie, Chen Yong, O'Neill Edward A, Engel Samuel S
Merck Research Laboratories, Merck & Co., Inc., Kenilworth, NJ, USA.
Real World Evidence and Epidemiology, GSK, Collegeville, PA, USA.
Diabetes Ther. 2018 Feb;9(1):309-315. doi: 10.1007/s13300-017-0360-6. Epub 2018 Jan 12.
Previous analyses concluded that patients initiating treatment with sitagliptin are older and have more comorbidities than patients initiating treatment with other oral antihyperglycemic agents (OAHAs). However, these studies focused on the general population or subjects ≤ 65 years of age. We sought to compare differences in baseline characteristics of elderly patients (≥ 65 years of age) with T2DM initiating sitagliptin vs. non-DPP-4 inhibitor (non-DPP-4i) OAHA in the MarketScan Medicare Supplemental Database.
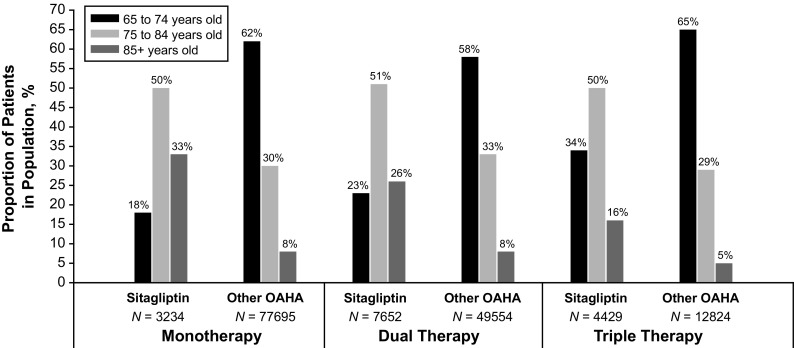
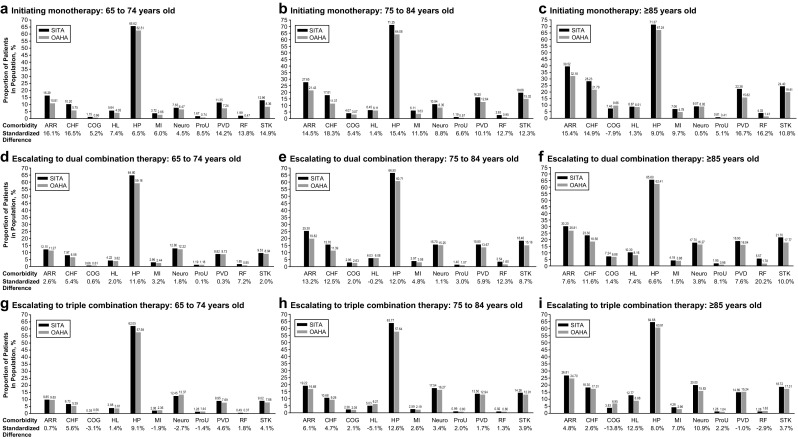
Relevant patients were identified in the MarketScan Medicare Supplemental Database and categorized according to the complexity of their antihyperglycemic treatment: initiating monotherapy, escalating to dual combination therapy, or escalating to triple combination therapy. Within each category, the comparison between patients initiating use of sitagliptin or non-DPP-4i OAHA was made within three age groups: 65-74, 75-84, and ≥ 85 years. Gender and comorbidity recorded within the 12 months prior to the index date (date of initiation/escalation of treatment) were assessed as baseline characteristics in each group. Between-treatment group differences in each covariate were compared using standardized differences.
Patients with T2DM who initiated treatment with sitagliptin tended to be older and were more likely to have a pre-treatment history of arrhythmia, congestive heart failure, peripheral vascular disease, renal failure, and stroke than those initiating non-DPP-4i OAHAs, with the most pronounced differences observed between patients initiating monotherapy in all three age groups. As treatment complexity advanced to dual combination therapy, the differences were attenuated and mostly observed in the 75-84 and ≥ 85 age groups. In patients aged 65-74 years initiating triple therapy, no differences were observed between groups.
Patients ≥ 65 years with T2DM initiating sitagliptin tend to be older and have more comorbidities than those prescribed other classes of OAHA. Appropriate adjustment is required to minimize the impact of potential confounding and channeling bias in any comparative analyses including users of sitagliptin.
Merck & Co., Inc., Kenilworth, NJ, USA.
先前的分析得出结论,与开始使用其他口服降糖药(OAHAs)治疗的患者相比,开始使用西格列汀治疗的患者年龄更大,合并症更多。然而,这些研究关注的是普通人群或年龄≤65岁的受试者。我们试图在MarketScan医疗保险补充数据库中比较老年2型糖尿病患者(≥65岁)开始使用西格列汀与非二肽基肽酶4抑制剂(non-DPP-4i)OAHAs的基线特征差异。
在MarketScan医疗保险补充数据库中识别相关患者,并根据其降糖治疗的复杂性进行分类:开始单药治疗、升级为双联联合治疗或升级为三联联合治疗。在每个类别中,在三个年龄组(65-74岁、75-84岁和≥85岁)内比较开始使用西格列汀或non-DPP-4i OAHAs的患者。将索引日期(治疗开始/升级日期)前12个月内记录的性别和合并症作为每组的基线特征。使用标准化差异比较各协变量在治疗组之间的差异。
与开始使用non-DPP-4i OAHAs的患者相比,开始使用西格列汀治疗的2型糖尿病患者往往年龄更大,并且更有可能有治疗前心律失常、充血性心力衰竭、外周血管疾病、肾衰竭和中风的病史,在所有三个年龄组中,开始单药治疗的患者之间观察到的差异最为明显。随着治疗复杂性进展到双联联合治疗,差异减弱,主要在75-84岁和≥85岁年龄组中观察到。在开始三联治疗的65-74岁患者中,各治疗组之间未观察到差异。
≥65岁开始使用西格列汀治疗的2型糖尿病患者往往比使用其他类OAHAs的患者年龄更大,合并症更多。在任何包括西格列汀使用者的比较分析中,都需要进行适当调整,以尽量减少潜在混杂和渠道偏倚的影响。
美国新泽西州肯尼沃思市默克公司。