Hanlon Peter, Nicholl Barbara I, Jani Bhautesh Dinesh, McQueenie Ross, Lee Duncan, Gallacher Katie I, Mair Frances S
General Practice and Primary Care, Institute of Health and Wellbeing, University of Glasgow, Glasgow, UK.
School of Mathematics and Statistics, University of Glasgow, Glasgow, UK.
BMJ Open. 2018 Jan 14;8(1):e018404. doi: 10.1136/bmjopen-2017-018404.
This study aims: (1) to describe the pattern and extent of multimorbidity and polypharmacy in UK Biobank participants with chronic obstructive pulmonary disease (COPD) and (2) to identify which comorbidities are associated with increased risk of adverse drug reactions (ADRs) resulting from polypharmacy.
Cross-sectional.
Community cohort.
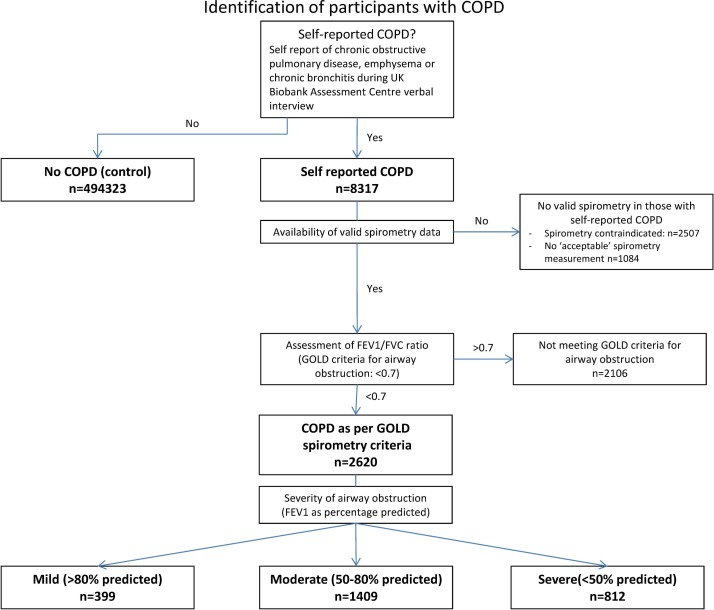
UK Biobank participants comparing self-reported COPD (n=8317) with no COPD (n=494 323).
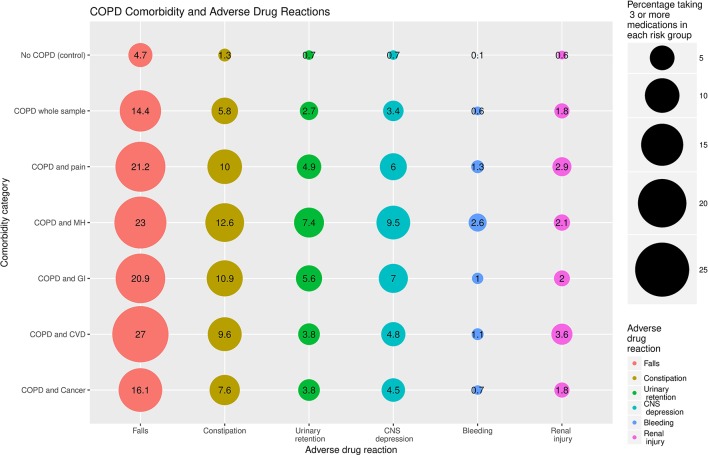
Multimorbidity (≥4 conditions) and polypharmacy (≥5 medications) in participants with COPD versus those without. Risk of ADRs (taking ≥3 medications associated with falls, constipation, urinary retention, central nervous system (CNS) depression, bleeding or renal injury) in relation to the presence of COPD and individual comorbidities.
Multimorbidity was more common in participants with COPD than those without (17% vs 4%). Polypharmacy was highly prevalent (52% with COPD taking ≥5 medications vs 18% in those without COPD). Adjusting for age, sex and socioeconomic status, those with COPD were significantly more likely than those without to be prescribed ≥3 medications contributing to falls (OR 2.27, 95% CI 2.13 to 2.42), constipation (OR 3.42, 95% CI 3.10 to 3.77), urinary retention (OR 3.38, 95% CI 2.94 to 3.87), CNS depression (OR 3.75, 95% CI 3.31 to 4.25), bleeding (OR 4.61, 95% CI 3.35 to 6.19) and renal injury (OR 2.22, 95% CI 1.86 to 2.62). Concomitant cardiovascular disease was associated with the greatest risk of taking ≥3 medications associated with falls/renal injury. Concomitant mental health conditions were most strongly associated with medications linked with CNS depression/urinary retention/bleeding.
Multimorbidity is common in COPD and associated with high levels of polypharmacy. Co-prescription of drugs with various ADRs is common. Future research should examine the effects on healthcare outcomes of co-prescribing multiple drugs with similar potential ADRs. Clinical guidelines should emphasise assessment of multimorbidity and ADR risk.
本研究旨在:(1)描述英国生物银行中慢性阻塞性肺疾病(COPD)参与者的共病模式和程度以及多重用药情况,(2)确定哪些合并症与多重用药导致的药物不良反应(ADR)风险增加相关。
横断面研究。
社区队列。
英国生物银行参与者,将自我报告患有COPD的参与者(n = 8317)与未患COPD的参与者(n = 494323)进行比较。
COPD患者的共病情况比非COPD患者更常见(17%对4%)。多重用药非常普遍(52%的COPD患者服用≥5种药物,而未患COPD的患者中这一比例为18%)。在调整年龄、性别和社会经济地位后,患有COPD的患者比未患COPD的患者更有可能被开具≥3种导致跌倒的药物(比值比[OR] 2.27,95%置信区间[CI] 2.13至2.42)、便秘药物(OR 3.42,95% CI 3.10至3.77)、尿潴留药物(OR 3.38,95% CI 2.94至3.87)、中枢神经系统(CNS)抑制药物(OR 3.75,95% CI 3.31至4.25)、出血药物(OR 4.61,95% CI 3.35至6.19)和肾损伤药物(OR 2.22,95% CI 1.86至2.62)。合并心血管疾病与服用≥3种与跌倒/肾损伤相关药物的风险最高相关。合并心理健康状况与与CNS抑制/尿潴留/出血相关的药物关联最为密切。
共病在COPD中很常见,并且与高水平的多重用药相关。具有各种ADR的药物联合处方很常见。未来的研究应考察联合开具具有相似潜在ADR的多种药物对医疗保健结果的影响。临床指南应强调对共病和ADR风险的评估。