Center for Clinical Epidemiology and Biostatistics, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Division of Gastroenterology, University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Am J Gastroenterol. 2018 Mar;113(3):405-417. doi: 10.1038/ajg.2017.479. Epub 2018 Jan 16.
Crohn's disease (CD) and ulcerative colitis (UC) are inflammatory bowel diseases (IBD) that compromise quality of life and may increase mortality. This study compared the mortality risk with prolonged corticosteroid use vs. antitumor necrosis factor-α (anti-TNF) drugs in IBD.
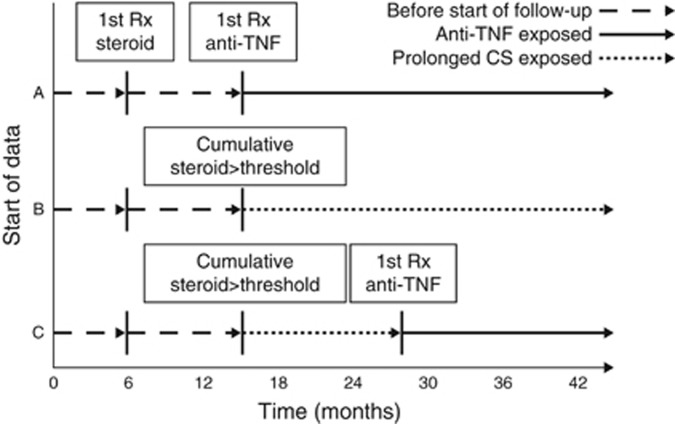
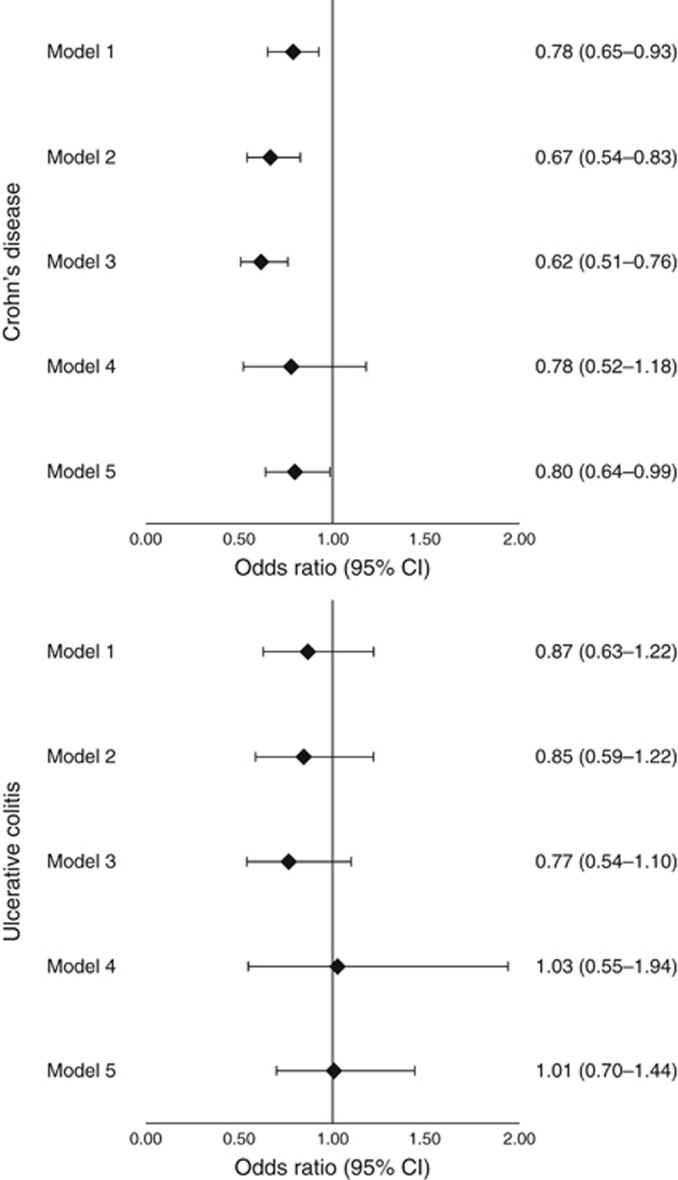
A retrospective cohort study was conducted among Medicaid and Medicare beneficiaries from 2001 to 2013 with IBD prescribed either >3,000 mg of prednisone or equivalent within a 12-month period or new initiation of anti-TNF therapy, each treated as time-updating exposures. The primary outcome was all-cause mortality. Secondary outcomes included common causes of death. Marginal structural models were used to determine odds ratios (ORs) and 95% confidence intervals (CIs) for anti-TNF use relative to corticosteroids.
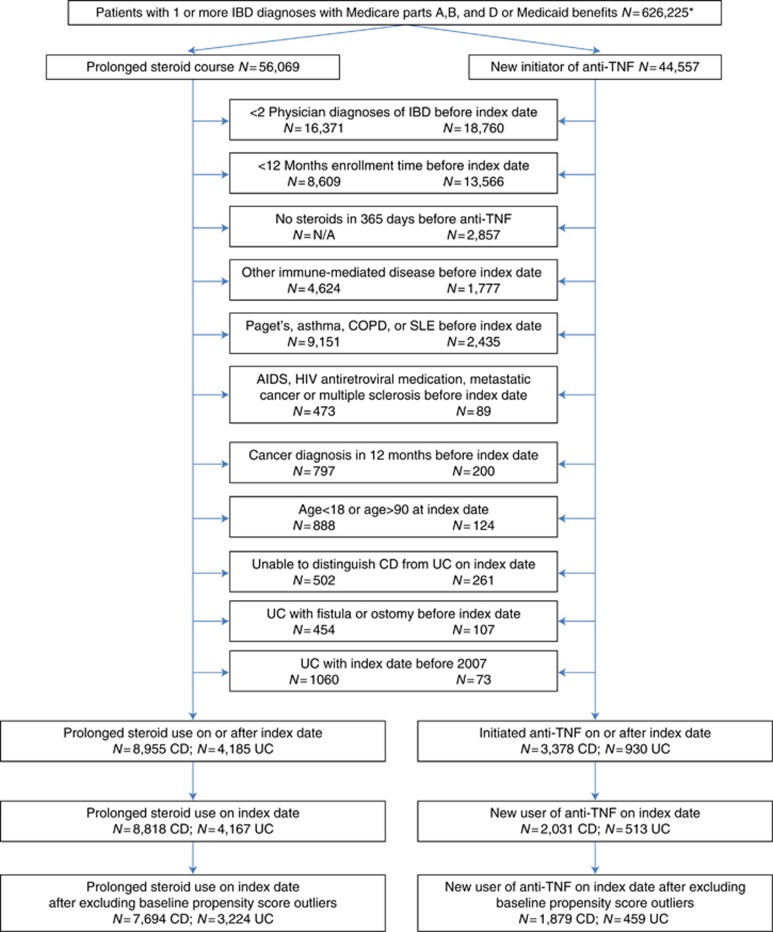
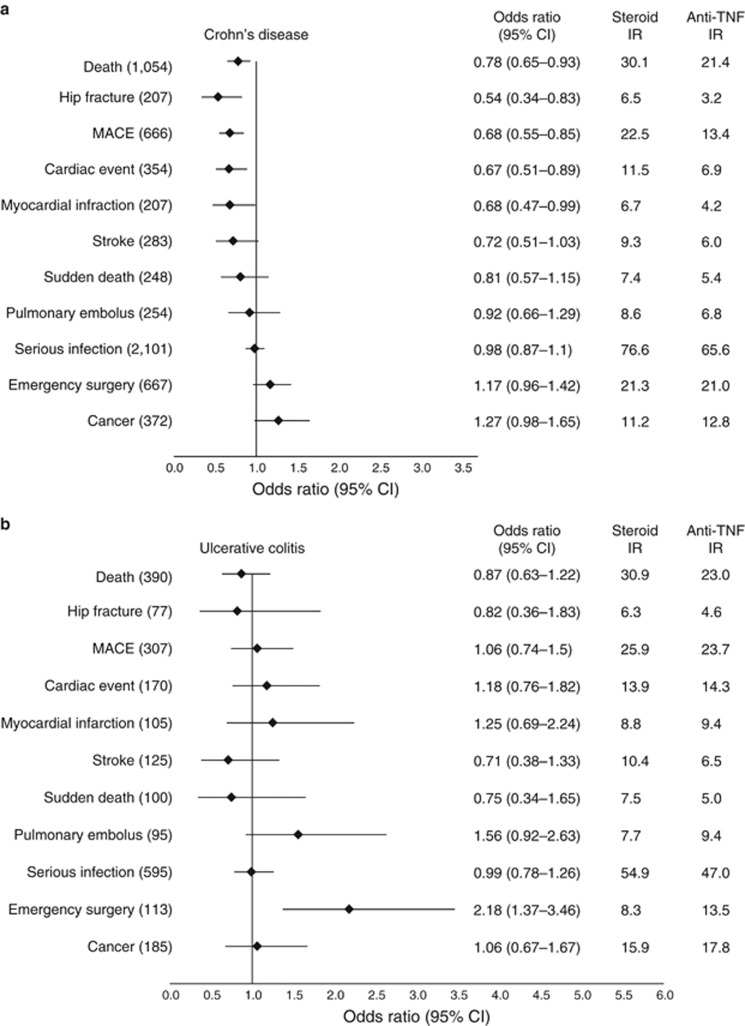
Among patients with CD, 7,694 entered the cohort as prolonged corticosteroid users and 1,879 as new anti-TNF users. Among patients with UC, 3,224 and 459 entered the cohort as prolonged CS users and new anti-TNF users, respectively. The risk of death was statistically significantly lower in patients treated with anti-TNF therapy for CD (21.4 vs. 30.1 per 1,000 person-years, OR 0.78, 0.65-0.93) but not for UC (23.0 vs. 30.9 per 1,000 person-years, OR 0.87, 0.63-1.22). Among the CD cohort, anti-TNF therapy was also associated with lower rates of major adverse cardiovascular events (OR 0.68, 0.55-0.85) and hip fracture (OR 0.54, 0.34-0.83).
Compared with prolonged corticosteroid exposure, anti-TNF drug use was associated with reduced mortality in patients with CD that may be explained by lower rates of major adverse cardiovascular events and hip fracture.
克罗恩病(CD)和溃疡性结肠炎(UC)是炎症性肠病(IBD),会降低生活质量并可能增加死亡率。本研究比较了 IBD 患者长期使用皮质类固醇与抗肿瘤坏死因子-α(anti-TNF)药物的死亡风险。
本研究是一项回顾性队列研究,纳入了 2001 年至 2013 年间接受 Medicaid 和 Medicare 保险的 IBD 患者,这些患者在 12 个月内接受了 >3000mg 泼尼松或等效药物治疗,或开始使用新的抗 TNF 治疗,这两种治疗方法均作为时间更新暴露因素。主要结局为全因死亡率。次要结局包括常见的死亡原因。使用边缘结构模型确定抗 TNF 治疗相对于皮质类固醇的比值比(OR)和 95%置信区间(CI)。
在 CD 患者中,7694 名患者进入了长期皮质类固醇使用者队列,1879 名患者进入了新的抗 TNF 使用者队列。在 UC 患者中,3224 名患者和 459 名患者分别进入了长期 CS 使用者队列和新的抗 TNF 使用者队列。CD 患者接受抗 TNF 治疗的死亡风险显著降低(21.4 比 30.1 每 1000 人年,OR 0.78,0.65-0.93),但 UC 患者无此结果(23.0 比 30.9 每 1000 人年,OR 0.87,0.63-1.22)。在 CD 队列中,抗 TNF 治疗还与较低的主要不良心血管事件发生率(OR 0.68,0.55-0.85)和髋部骨折发生率(OR 0.54,0.34-0.83)相关。
与长期皮质类固醇暴露相比,抗 TNF 药物的使用与 CD 患者的死亡率降低相关,这可能是由于主要不良心血管事件和髋部骨折的发生率降低所致。