Department of Orthopedics and Sports Orthopedics, Technical University of Munich, 81547, Munich, Germany.
Sportmedizin Zürich, Schulthess Klinik, Zurich, Switzerland.
Eur J Med Res. 2018 Jan 16;23(1):5. doi: 10.1186/s40001-018-0302-4.
Several surgical options for the reconstruction of massive bone defects have been described and include biologic methods with autografts and allografts, and the use of tumor endoprostheses (total femoral replacement, TFR). Several types of modular TFR are available, but nevertheless unpredictable outcomes and high complication rates have been described from most authors. The present study aims to compare results after TFR performed with modular total femur prosthesis MML (Fa. ESKA/Orthodynamics) in patients with and without malignant disease.
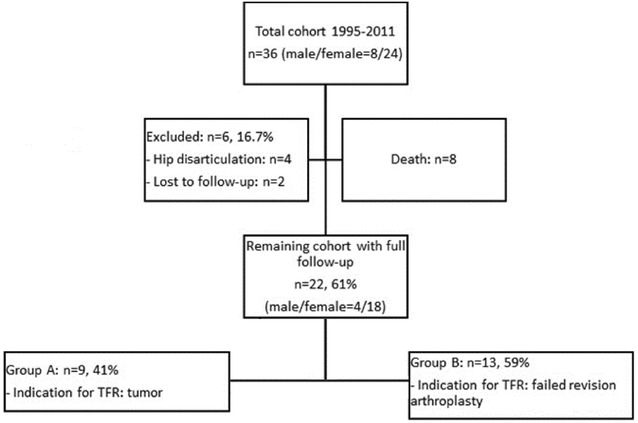
Retrospective chart review and functional investigation (Musculoskeletal Tumor Society (MSTS) score, Harris Hip Score (HHS), Oxford Knee Score (OKS), SF-12 Health Survey, and failure classification according to Henderson) of TFR cases from 1995 to 2011. Indications for TFR were malignant tumor resection from the femur (n = 9, Group A) or failure of a revision arthroplasty without history of malignant disease (n = 13, Group B).
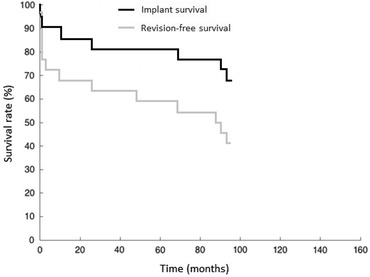
Thirty-six patients were treated during the study period, of whom 22 could be investigated clinically after a mean follow-up of 63 months. Overall failure rate for TFR was 59.1%, leading to 38 surgical revisions. The most common failure mechanisms were Type I (soft tissue), followed by Type IV (infection) and Type III (mechanical failure). Mean MSTS score out of 30 was 13 (range 1-25), with significantly higher scores in Group A (mean 19, range 3-25) than Group B (mean 9, range 1-15).
TFR is an established procedure to restore femoral integrity. However, complication rates are considerably high, and depend mainly on the age at initial reconstruction.
已经描述了几种用于重建大骨缺损的手术选择,包括使用自体移植物和同种异体移植物的生物方法,以及使用肿瘤假体(全股骨置换,TFR)。有几种类型的模块化 TFR 可用,但大多数作者都描述了不可预测的结果和高并发症发生率。本研究旨在比较在患有和不患有恶性疾病的患者中使用模块化全股骨假体 MML(Fa. ESKA/Orthodynamics)进行 TFR 的结果。
回顾性图表审查和功能调查(肌肉骨骼肿瘤学会(MSTS)评分、Harris 髋关节评分(HHS)、牛津膝关节评分(OKS)、SF-12 健康调查以及根据 Henderson 进行的失败分类)1995 年至 2011 年的 TFR 病例。TFR 的指征是股骨恶性肿瘤切除(n=9,A 组)或无恶性疾病病史的翻修关节置换失败(n=13,B 组)。
在研究期间,有 36 名患者接受了治疗,其中 22 名在平均随访 63 个月后进行了临床调查。TFR 的总体失败率为 59.1%,导致 38 次手术修订。最常见的失败机制是 I 型(软组织),其次是 IV 型(感染)和 III 型(机械故障)。30 分的平均 MSTS 评分为 13(范围 1-25),A 组(平均 19,范围 3-25)明显高于 B 组(平均 9,范围 1-15)。
TFR 是一种重建股骨完整性的既定手术方法。然而,并发症发生率相当高,主要取决于初始重建时的年龄。