Yoshihisa Akiomi, Kanno Yuki, Watanabe Shunsuke, Yokokawa Tetsuro, Abe Satoshi, Miyata Makiko, Sato Takamasa, Suzuki Satoshi, Oikawa Masayoshi, Kobayashi Atsushi, Yamaki Takayoshi, Kunii Hiroyuki, Nakazato Kazuhiko, Suzuki Hitoshi, Ishida Takafumi, Takeishi Yasuchika
Department of Cardiovascular Medicine, Fukushima Kenritsu Ika Daigaku, Fukushima, Japan.
Open Heart. 2018 Jan 9;5(1):e000730. doi: 10.1136/openhrt-2017-000730. eCollection 2018.
Malnutrition is a common condition that is associated with adverse prognosis in patients with heart failure (HF). The Prognostic Nutritional Index (PNI), Geriatric Nutritional Risk Index (GNRI) and controlling nutritional status (CONUT) have all been used as objective indices for evaluating nutritional status. We aimed to clarify the relationship between these nutritional indices and the parameters of inflammatory markers, cardiac function and exercise capacity, as well as to compare the ability of these indexes for predicting mortality.
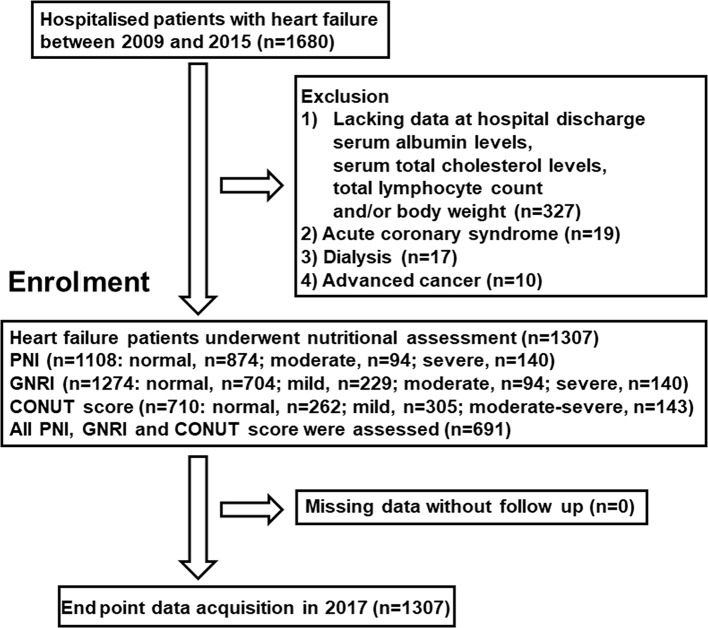
We evaluated PNI, GNRI and CONUT in consecutive 1307 patients with HF.
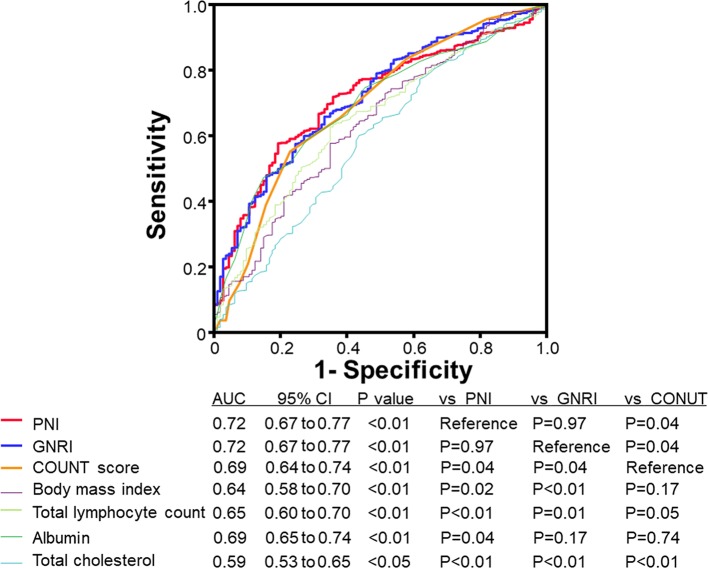
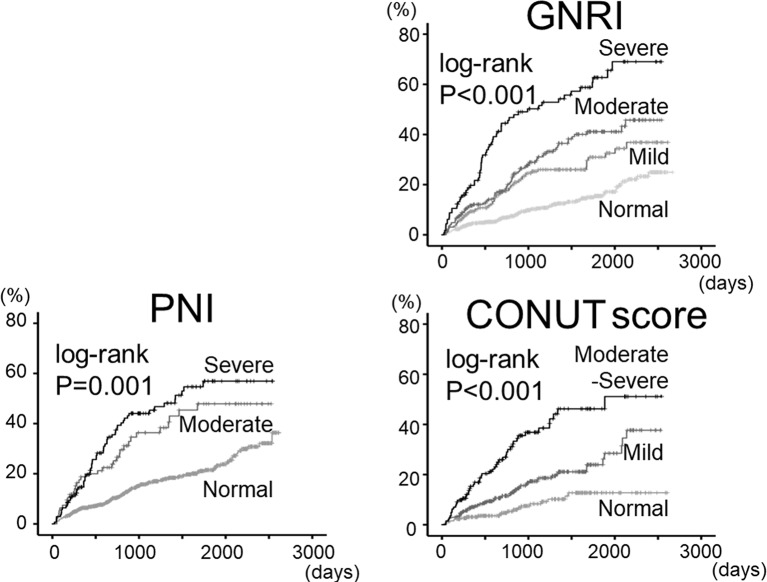
First, there were significant correlations between nutritional indices and the following: C reactive protein; tumour necrosis factor-α; adiponectin; B-type natriuretic peptide; troponin I; inferior vena cava diameter and peak VO (P<0.05, respectively). Second, in the Kaplan-Meier analysis (follow-up 1146 days), all-cause mortality progressively increased from normal to mild, moderate and severe disturbance groups in the indices (log-rank, P<0.01, respectively). In the Cox proportional hazard analysis, each index was an independent predictor of all-cause mortality in patients with HF (P<0.001, respectively). Third, receiver operating curve demonstrated that the areas under the curve of PNI and GNRI were larger than that of CONUT score (P<0.05, respectively).
Patients with HF being malnourished had higher mortality accompanied by higher levels of C reactive protein, tumour necrosis factor-α, adiponectin, B-type natriuretic peptide, troponin I, right-sided volume overload and impaired exercise capacity, rather than left ventricular systolic function. Additionally, PNI and GNRI were superior to CONUT score in predicting mortality in patients with HF.
营养不良是一种常见情况,与心力衰竭(HF)患者的不良预后相关。预后营养指数(PNI)、老年营养风险指数(GNRI)和控制营养状况(CONUT)均已被用作评估营养状况的客观指标。我们旨在阐明这些营养指标与炎症标志物、心功能和运动能力参数之间的关系,并比较这些指标预测死亡率的能力。
我们对连续1307例HF患者评估了PNI、GNRI和CONUT。
首先,营养指标与以下各项之间存在显著相关性:C反应蛋白;肿瘤坏死因子-α;脂联素;B型利钠肽;肌钙蛋白I;下腔静脉直径和峰值VO(分别P<0.05)。其次,在Kaplan-Meier分析(随访1146天)中,全因死亡率在各指标中从正常组到轻度、中度和重度紊乱组逐渐增加(对数秩检验,分别P<0.01)。在Cox比例风险分析中,每个指标都是HF患者全因死亡率的独立预测因子(分别P<0.001)。第三,受试者工作特征曲线显示,PNI和GNRI的曲线下面积大于CONUT评分的曲线下面积(分别P<0.05)。
HF营养不良患者死亡率较高,同时伴有较高水平的C反应蛋白、肿瘤坏死因子-α、脂联素、B型利钠肽、肌钙蛋白I、右心容量超负荷和运动能力受损,而非左心室收缩功能受损。此外,在预测HF患者死亡率方面,PNI和GNRI优于CONUT评分。