Medizinische Klinik V and.
Institute of Human Genetics, University Hospital of Heidelberg, Heidelberg, Germany.
Blood Adv. 2017 Dec 27;2(1):1-9. doi: 10.1182/bloodadvances.2017013334. eCollection 2018 Jan 9.
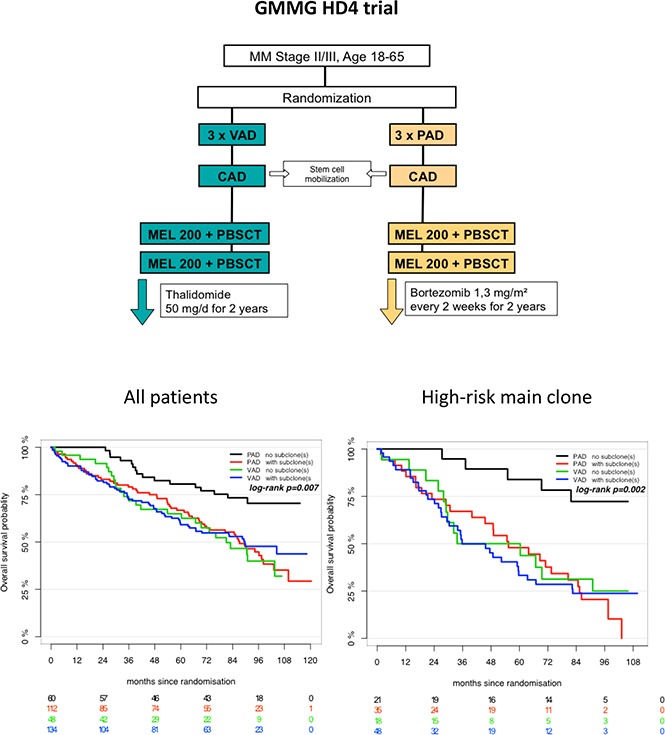
We investigated subclonal cytogenetic aberrations (CA) detected by interphase fluorescence in situ hybridization (iFISH) in patients with newly diagnosed multiple myeloma (MM) enrolled in the Haemato Oncology Foundation for Adults in the Netherlands (HOVON)-65/German-Speaking MM Group (GMMG)-HD4 phase 3 trial. Patients were either treated with 3 cycles of vincristine, Adriamycin, and dexamethasone or bortezomib, Adriamycin, and dexamethasone and then thalidomide or bortezomib maintenance after tandem autologous transplantation. Subclones were defined either by presence of different copy numbers of the same chromosome loci and/or CA present in at least 30% less and maximally 2/3 of cells compared with the main clone CA. Patients with subclones harbored more frequently high risk (31.0%) or hyperdiploid main clone aberrations (24.8%) than patients with t(11;14) in the main clone (10.1%). Gains and deletions of c-MYC were the only CA that occurred more frequently as subclone (8.1%/20.5%) than main clone (6.2%/3.9%, respectively). Treatment with bortezomib completely overcame the negative prognosis of high-risk CA in patients without subclones, but not in patients with additional subclonal CA. High-risk patients treated without bortezomib showed dismal outcome whether subclones were present or not. Cytogenetic heterogeneity defined by subclonal CA is of major prognostic significance in newly diagnosed MM patients treated with bortezomib within the HOVON-65/GMMG-HD4 trial.
我们研究了荷兰成人血液肿瘤基金会(HOVON)-65/德语骨髓瘤组(GMMG)-HD4 期 3 试验中新诊断多发性骨髓瘤(MM)患者间期荧光原位杂交(iFISH)检测到的亚克隆细胞遗传学异常(CA)。患者接受 3 周期长春新碱、阿霉素和地塞米松或硼替佐米、阿霉素和地塞米松治疗,然后在自体移植后进行沙利度胺或硼替佐米维持治疗。亚克隆通过相同染色体位点数目的不同拷贝数或与主克隆 CA 相比,至少 30%减少且最多 2/3 细胞存在的 CA 来定义。与主克隆 t(11;14)相比,存在亚克隆的患者更常出现高危(31.0%)或超二倍体主克隆异常(24.8%)。主克隆中 c-MYC 的增益和缺失是唯一比主克隆更常作为亚克隆(8.1%/20.5%)出现的 CA(分别为 6.2%/3.9%)。在没有亚克隆的患者中,硼替佐米的治疗完全克服了高危 CA 的不良预后,但在存在额外亚克隆 CA 的患者中则不然。无论是否存在亚克隆,未接受硼替佐米治疗的高危患者预后均不佳。在 HOVON-65/GMMG-HD4 试验中,用硼替佐米治疗的新诊断 MM 患者中,亚克隆 CA 定义的细胞遗传学异质性具有重要的预后意义。