Centre for Clinical Research, Faculty of Medicine, The University of Queensland, Brisbane, Australia.
QIMR Berghofer Medical Research Institute, Brisbane, Australia.
J Pathol. 2018 Apr;244(4):460-468. doi: 10.1002/path.5040. Epub 2018 Mar 9.
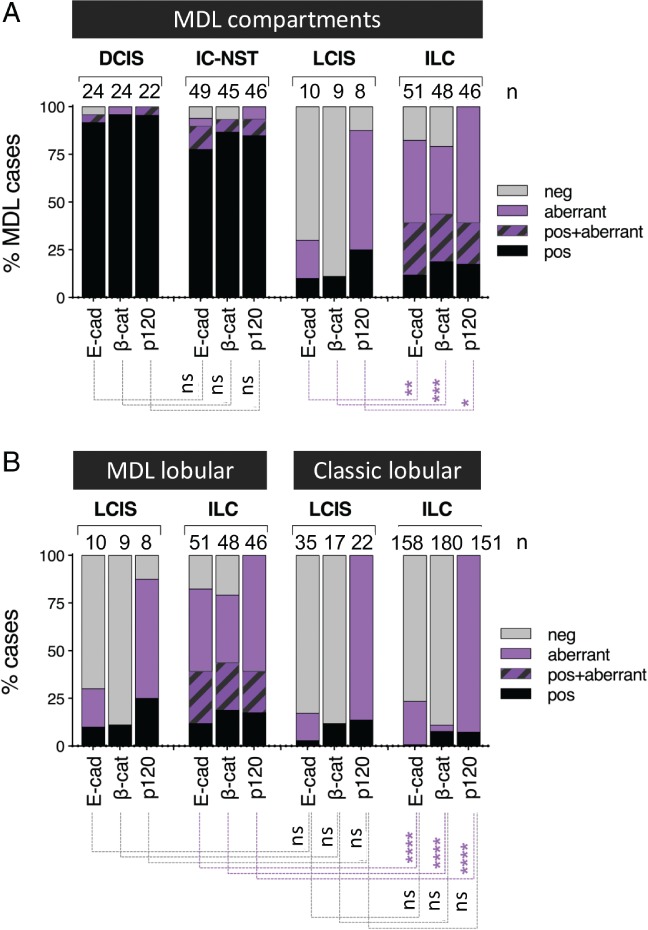
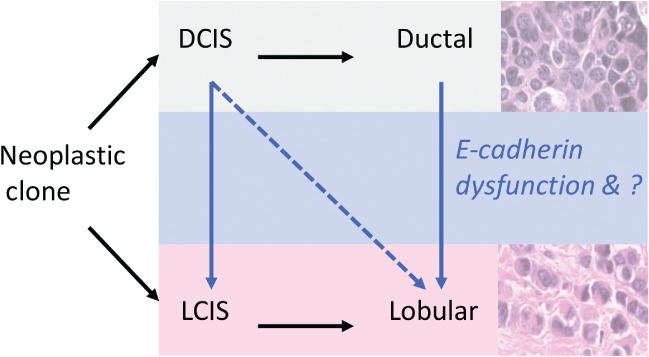
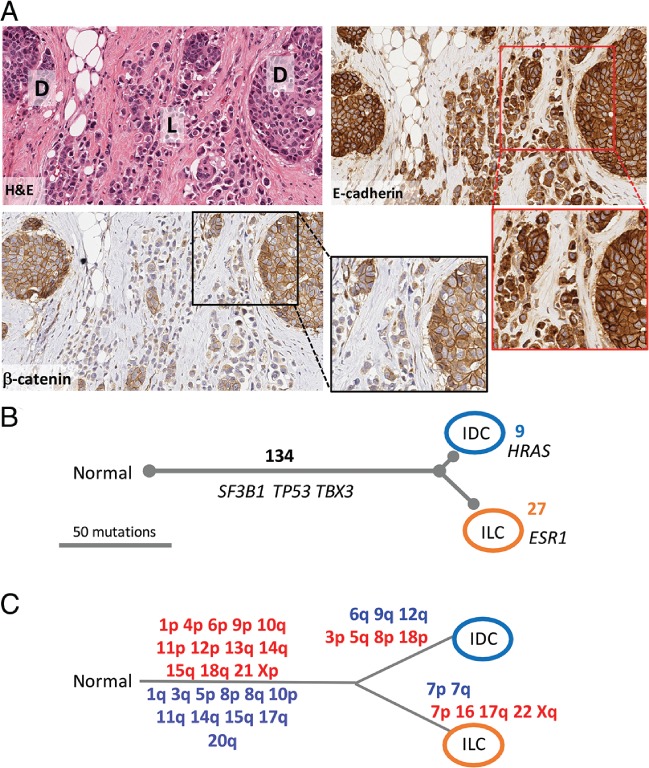
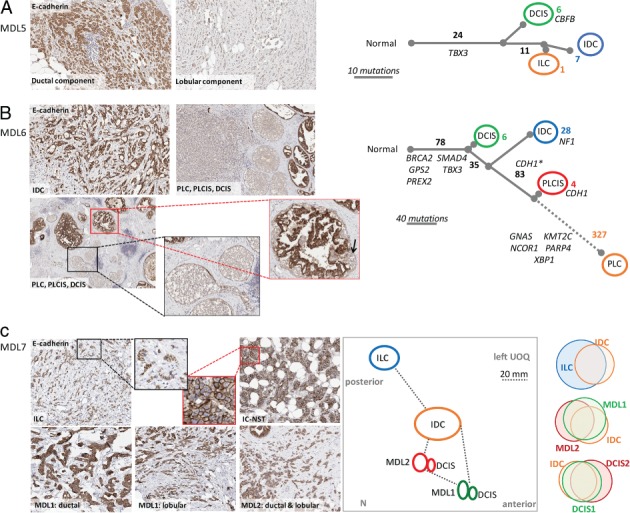
Mixed ductal-lobular carcinomas (MDLs) show both ductal and lobular morphology, and constitute an archetypal example of intratumoural morphological heterogeneity. The mechanisms underlying the coexistence of these different morphological entities are poorly understood, although theories include that these components either represent 'collision' of independent tumours or evolve from a common ancestor. We performed comprehensive clinicopathological analysis of a cohort of 82 MDLs, and found that: (1) MDLs more frequently coexist with ductal carcinoma in situ (DCIS) than with lobular carcinoma in situ (LCIS); (2) the E-cadherin-catenin complex was normal in the ductal component in 77.6% of tumours; and (3) in the lobular component, E-cadherin was almost always aberrantly located in the cytoplasm, in contrast to invasive lobular carcinoma (ILC), where E-cadherin is typically absent. Comparative genomic hybridization and multiregion whole exome sequencing of four representative cases revealed that all morphologically distinct components within an individual case were clonally related. The mutations identified varied between cases; those associated with a common clonal ancestry included BRCA2, TBX3, and TP53, whereas those associated with clonal divergence included CDH1 and ESR1. Together, these data support a model in which separate morphological components of MDLs arise from a common ancestor, and lobular morphology can arise via a ductal pathway of tumour progression. In MDLs that present with LCIS and DCIS, the clonal divergence probably occurs early, and is frequently associated with complete loss of E-cadherin expression, as in ILC, whereas, in the majority of MDLs, which present with DCIS but not LCIS, direct clonal divergence from the ductal to the lobular phenotype occurs late in tumour evolution, and is associated with aberrant expression of E-cadherin. The mechanisms driving the phenotypic change may involve E-cadherin-catenin complex deregulation, but are yet to be fully elucidated, as there is significant intertumoural heterogeneity, and each case may have a unique molecular mechanism. © 2018 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
混合导管-小叶性癌(MDL)同时具有导管和小叶形态,是肿瘤内形态异质性的典型范例。尽管存在这些成分代表“碰撞”的独立肿瘤或从共同祖先进化而来的理论,但对于导致这些不同形态实体共存的机制仍知之甚少。我们对 82 例 MDL 队列进行了全面的临床病理分析,发现:(1)MDL 与导管原位癌(DCIS)共存的频率高于与小叶原位癌(LCIS)共存;(2)77.6%的肿瘤中,导管成分的 E-钙粘蛋白-连环蛋白复合物是正常的;(3)在小叶成分中,E-钙粘蛋白几乎总是异常定位于细胞质中,与浸润性小叶癌(ILC)相反,E-钙粘蛋白通常不存在。对四个代表性病例的比较基因组杂交和多区域全外显子组测序显示,单个病例中所有形态不同的成分在克隆上均相关。鉴定的突变在病例之间有所不同;与共同克隆起源相关的突变包括 BRCA2、TBX3 和 TP53,而与克隆分化相关的突变包括 CDH1 和 ESR1。总之,这些数据支持这样一种模型,即 MDL 的不同形态成分源自共同的祖先,小叶形态可以通过肿瘤进展的导管途径产生。在同时具有 LCIS 和 DCIS 的 MDL 中,克隆分化可能发生得更早,并且经常与 E-钙粘蛋白表达完全丧失相关,如在 ILC 中,而在大多数同时具有 DCIS 但不具有 LCIS 的 MDL 中,导管到小叶表型的直接克隆分化发生在肿瘤进化的晚期,与 E-钙粘蛋白的异常表达相关。驱动表型变化的机制可能涉及 E-钙粘蛋白-连环蛋白复合物的失调,但尚未完全阐明,因为存在显著的肿瘤间异质性,并且每个病例可能具有独特的分子机制。© 2018 作者。约翰威立父子公司代表英国和爱尔兰病理学学会出版的《病理学杂志》。