Gjesdal Grunde, Braun Oscar Ö, Smith J Gustav, Scherstén Fredrik, Tydén Patrik
Department of Cardiology, Clinical Sciences, Lund University and Skåne University Hospital, SE-221 81, Lund, Sweden.
BMC Cardiovasc Disord. 2018 Jan 18;18(1):8. doi: 10.1186/s12872-018-0744-1.
Mortality in patients with acute myocardial infarction (AMI) has improved substantially with modern therapy including percutaneous coronary interventions (PCI) but remains high in certain subgroups such as patients presenting with overt cardiogenic shock. However, the risk for AMI in patients presenting acutely with signs of heart failure but without cardiogenic shock is less well described. We aimed to identify risk factors for mortality in AMI patients with heart failure without overt cardiogenic shock.
Using data from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR), we identified patients with operator-registered heart failure (Killip class II-IV), and evaluated predictors of mortality based on clinical factors from review of patient records.
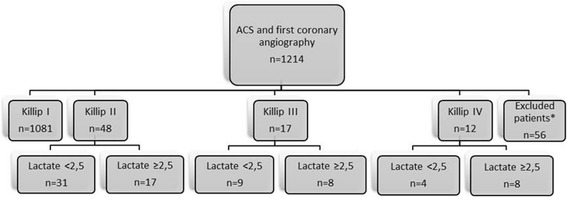
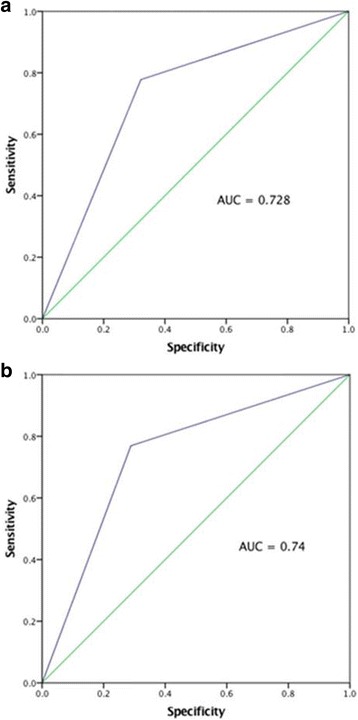
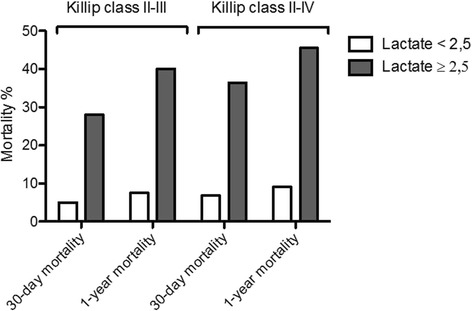
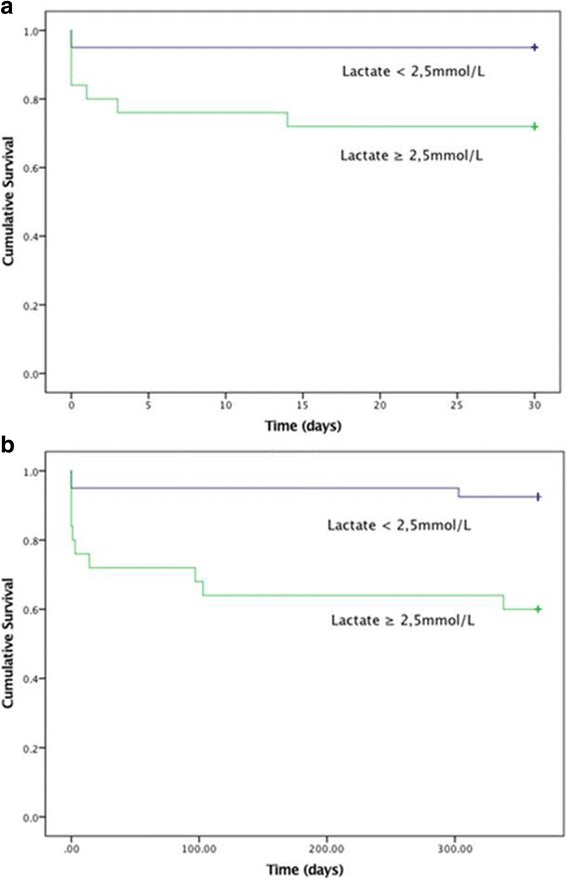
A total of 1260 unique patients with acute myocardial infarction underwent PCI in 2014, of which 77 patients (7%) showed signs of heart failure (Killip II-IV) Overall 30-day mortality in patients with Killip class II-IV was 20% (N = 15). In patients classified Killip IV (1%), 30-day mortality was 50% (N = 6). In patients presenting with mild to moderate heart failure (Killlip class II-III), 30-day mortality was 14% (N = 9). In patients with Killip class II-III, lactate ≥2.5 mmol/L was associated with 30-day mortality, whereas systolic blood pressure < 90 mmHg, age, sex and BMI were not. In patients with lactate < 2.5 mmol/L 30-day mortality was 5% (N = 2) whereas mortality was 28% (N = 7) with lactate ≥2.5 mmol/L. This cut-off provided discriminative information on 30-day mortality (area under ROC curve 0.74).
In patients with AMI and signs of mild to moderate heart failure, lactate ≥2.5 mmol/L provides additional prognostic information. Interventions to reduce risk may be targeted to these patients.
急性心肌梗死(AMI)患者的死亡率通过包括经皮冠状动脉介入治疗(PCI)在内的现代治疗方法已大幅改善,但在某些亚组中,如出现明显心源性休克的患者,死亡率仍然很高。然而,急性出现心力衰竭症状但无心源性休克的患者发生AMI的风险描述较少。我们旨在确定无明显心源性休克的AMI合并心力衰竭患者的死亡危险因素。
利用瑞典冠状动脉造影和血管成形术登记处(SCAAR)的数据,我们确定了经操作者登记的心力衰竭(Killip分级II-IV级)患者,并根据患者记录回顾中的临床因素评估死亡预测因素。
2014年共有1260例急性心肌梗死患者接受了PCI,其中77例(7%)出现心力衰竭症状(Killip II-IV级)。Killip II-IV级患者的30天总死亡率为20%(N = 15)。Killip IV级(1%)患者的30天死亡率为50%(N = 6)。轻度至中度心力衰竭(Killlip分级II-III级)患者的30天死亡率为14%(N = 9)。在Killip II-III级患者中,乳酸≥2.5 mmol/L与30天死亡率相关,而收缩压<90 mmHg、年龄、性别和BMI则无关。乳酸<2.5 mmol/L的患者30天死亡率为5%(N = 2),而乳酸≥2.5 mmol/L的患者死亡率为28%(N = 7)。这一切点提供了关于30天死亡率的鉴别信息(ROC曲线下面积为0.74)。
在AMI合并轻度至中度心力衰竭症状的患者中,乳酸≥2.5 mmol/L提供了额外的预后信息。降低风险的干预措施可针对这些患者。