Institute of Health and Society, Sir James Spence Institute, Royal Victoria Infirmary, Newcastle University, Newcastle upon Tyne, NE1 4LP, UK.
NIHR Health Protection Research Unit in Chemical and Radiation Threats and Hazards, Newcastle University, Newcastle upon Tyne, NE2 4AA, UK.
Eur J Epidemiol. 2018 Apr;33(4):393-401. doi: 10.1007/s10654-018-0357-0. Epub 2018 Jan 18.
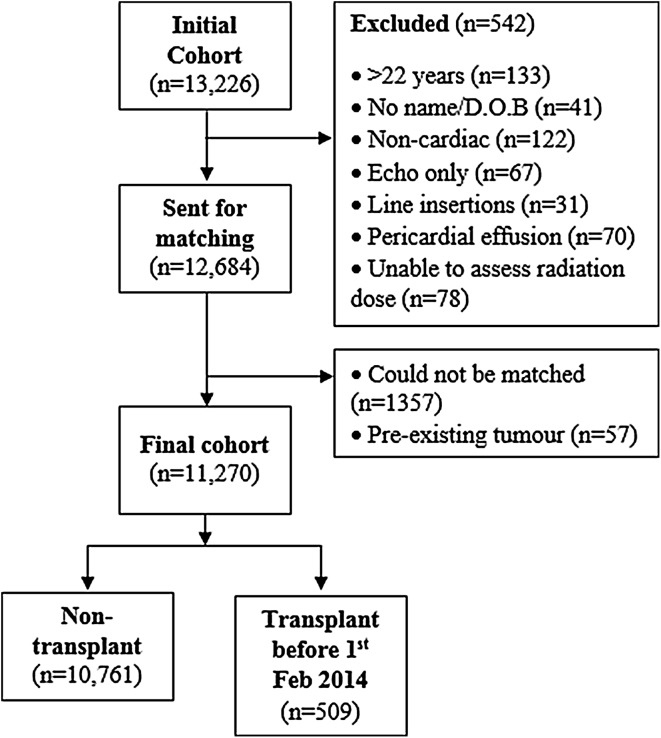
Children and young adults with heart disease appear to be at increased risk of developing cancer, although the reasons for this are unclear. A cohort of 11,270 individuals, who underwent cardiac catheterizations while aged ≤ 22 years in the UK, was established from hospital records. Radiation doses from cardiac catheterizations and CT scans were estimated. The cohort was matched with the NHS Central Register and NHS Transplant Registry to determine cancer incidence and transplantation status. Standardized incidence ratios (SIR) with associated confidence intervals (CI) were calculated. The excess relative risk (ERR) of lymphohaematopoietic neoplasia was also calculated using Poisson regression. The SIR was raised for all malignancies (2.32, 95% CI 1.65, 3.17), lymphoma (8.34, 95% CI 5.22, 12.61) and leukaemia (2.11, 95% CI 0.82, 4.42). After censoring transplant recipients, post-transplant, the SIR was reduced to 0.90 (95% CI 0.49, 1.49) for all malignancies. All lymphomas developed post-transplant. The SIR for all malignancies developing 5 years from the first cardiac catheterization (2 years for leukaemia/lymphoma) remained raised (3.01, 95% CI 2.09, 4.19) but was again reduced after censoring transplant recipients (0.98, 95% CI 0.48, 1.77). The ERR per mGy bone marrow dose for lymphohaematopoietic neoplasia was reduced from 0.541 (95% CI 0.104, 1.807) to 0.018 (95% CI - 0.002, 0.096) where transplantation status was accounted for as a time-dependent background risk factor. In conclusion, transplantation appears to be a large contributor to elevated cancer rates in this patient group. This is likely to be mainly due to associated immunosuppression, however, radiation exposure may also be a contributing factor.
儿童和青少年心脏病患者似乎患癌症的风险增加,尽管其原因尚不清楚。该队列纳入了 11270 名在英国年龄≤22 岁时接受过心脏导管检查的患者,其数据来源于医院记录。评估了心脏导管检查和 CT 扫描的辐射剂量。通过与英国国家医疗服务体系(NHS)中央登记处和 NHS 移植登记处进行匹配,确定癌症发病率和移植情况。计算了标准化发病率比(SIR)及其置信区间(CI)。还使用泊松回归计算了淋巴造血系统肿瘤的超额相对风险(ERR)。所有恶性肿瘤(2.32,95%CI 1.65,3.17)、淋巴瘤(8.34,95%CI 5.22,12.61)和白血病(2.11,95%CI 0.82,4.42)的 SIR 均升高。在排除移植受者后,移植后所有恶性肿瘤的 SIR 降低至 0.90(95%CI 0.49,1.49)。所有淋巴瘤均在移植后发生。首次心脏导管检查后 5 年(白血病/淋巴瘤为 2 年)发生的所有恶性肿瘤的 SIR 仍然升高(3.01,95%CI 2.09,4.19),但在排除移植受者后再次降低(0.98,95%CI 0.48,1.77)。考虑到移植状态是一个随时间变化的背景风险因素,骨髓剂量每增加 1mGy 时,淋巴造血系统肿瘤的 ERR 从 0.541(95%CI 0.104,1.807)降至 0.018(95%CI -0.002,0.096)。总之,移植似乎是导致该患者群体癌症发病率升高的一个重要因素。这很可能主要归因于相关的免疫抑制,但辐射暴露也可能是一个促成因素。