Yamamoto Takayuki, Okada Tomohisa, Fushimi Yasutaka, Yamamoto Akira, Fujimoto Koji, Okuchi Sachi, Fukutomi Hikaru, Takahashi Jun C, Funaki Takeshi, Miyamoto Susumu, Stalder Aurélien F, Natsuaki Yutaka, Speier Peter, Togashi Kaori
Department of Diagnostic Imaging and Nuclear Medicine, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
Department of Neurosurgery, National Cerebral and Cardiovascular Center, Suita, Japan.
PLoS One. 2018 Jan 19;13(1):e0189493. doi: 10.1371/journal.pone.0189493. eCollection 2018.
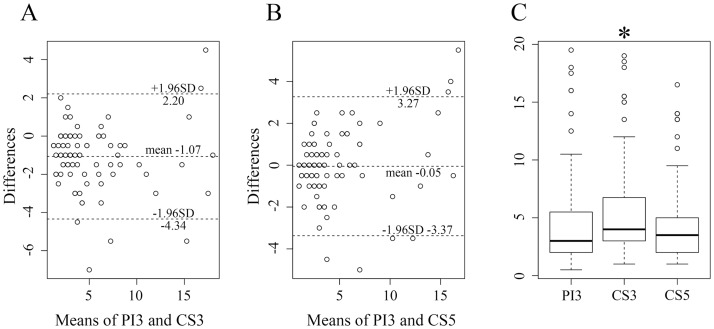
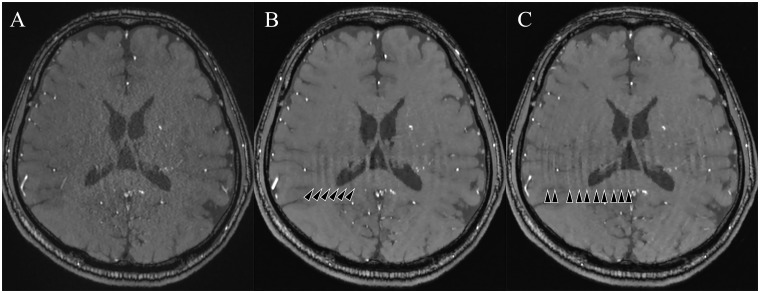
Compressed sensing (CS) reconstructions of under-sampled measurements generate missing data based on assumptions of image sparsity. Non-contrast time-of-flight MR angiography (TOF-MRA) is a good candidate for CS based acceleration, as MRA images feature bright trees of sparse vessels over a well-suppressed anatomical background signal. A short scan time derived from CS is beneficial for patients of moyamoya disease (MMD) because of the frequency of MR scans. The purpose of this study was to investigate the reliability of TOF-MRA with CS in the evaluation of MMD. Twenty-two patients were examined using TOF-MRA with CS (CS-TOF) and parallel imaging (PI-TOF). The acceleration factors were 3 (CS3) and 5 (CS5) for CS-TOF, and 3 (PI3) for PI-TOF. Two neuroradiologists evaluated the MMD grading according to stenosis/occlusion scores using the modified Houkin's system, and the visibility of moyamoya vessels (MMVs) using a 3-point scale. Concordance was calculated with Cohen's κ. The numbers of MMVs in the basal ganglia were compared using Bland-Altman analysis and Wilcoxon's signed-rank tests. MRA scan times were 4:07, 3:53, and 2:42 for PI3, CS3, and CS5, respectively. CS-reconstruction completed within 10 minutes. MMD grading and MMV visibility scales showed excellent correlation (κ > .966). Although the number of MMVs was significantly higher in CS3 than in PI3 (p < .0001) and CS5 (p < .0001), Bland-Altman analysis showed a good agreement between PI3, CS3, and CS5. Compressed sensing can accelerate TOF-MRA with improved visualization of small collaterals in equivalent time (CS3) or equivalent results in a shorter scan time (CS5).
基于图像稀疏性假设,对欠采样测量值进行压缩感知(CS)重建会生成缺失数据。非对比时间飞跃磁共振血管造影(TOF-MRA)是基于CS加速的理想选择,因为MRA图像在充分抑制的解剖背景信号上呈现出稀疏血管的明亮树状结构。由于MR扫描的频率,CS带来的短扫描时间对烟雾病(MMD)患者有益。本研究的目的是探讨CS-TOF-MRA在MMD评估中的可靠性。对22例患者进行了CS-TOF-MRA和并行成像(PI-TOF)检查。CS-TOF的加速因子为3(CS3)和5(CS5),PI-TOF的加速因子为3(PI3)。两名神经放射科医生根据改良的Houkin系统,使用狭窄/闭塞评分评估MMD分级,并使用3分制评估烟雾病血管(MMV)的可视性。使用Cohen's κ计算一致性。使用Bland-Altman分析和Wilcoxon符号秩检验比较基底节区MMV的数量。PI3、CS3和CS5的MRA扫描时间分别为4:07、3:53和2:42。CS重建在10分钟内完成。MMD分级和MMV可视性量表显示出极好的相关性(κ>.966)。虽然CS3中MMV的数量显著高于PI3(p<.0001)和CS5(p<.0001),但Bland-Altman分析显示PI3、CS3和CS5之间具有良好的一致性。压缩感知可以加速TOF-MRA,在相同时间(CS3)内改善小侧支的可视化,或在更短的扫描时间内获得等效结果(CS5)。