Department of Hematology, Cliniques Universitaires Saint-Luc, UCL Brussels, Belgium.
Hematology Department, CHU UCL Namur, Yvoir, Belgium.
Haematologica. 2018 May;103(5):840-848. doi: 10.3324/haematol.2017.180554. Epub 2018 Jan 19.
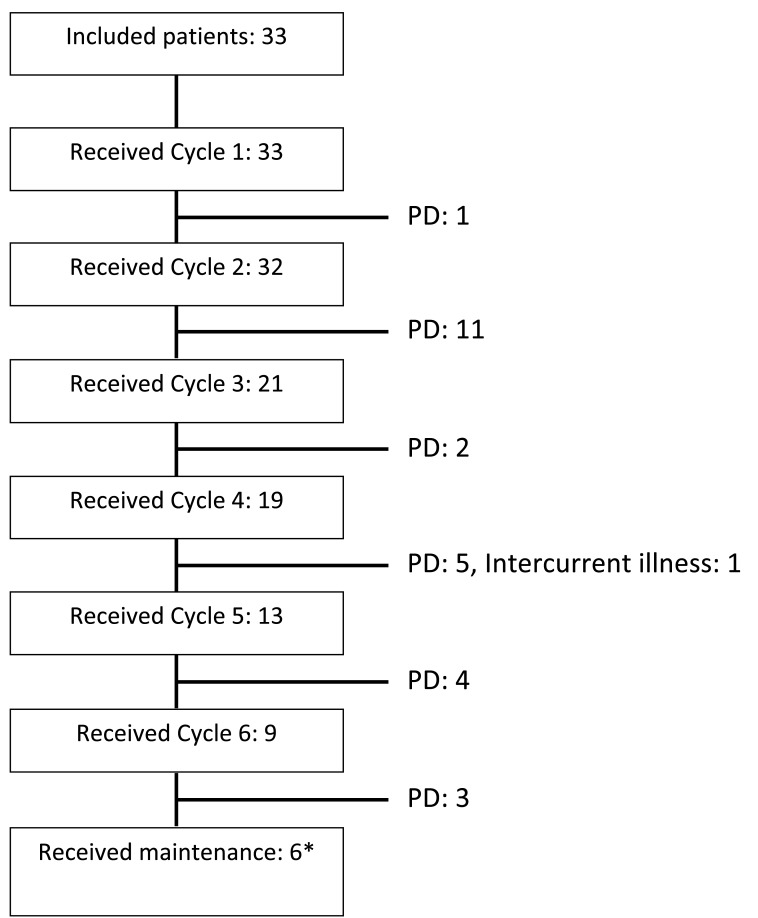
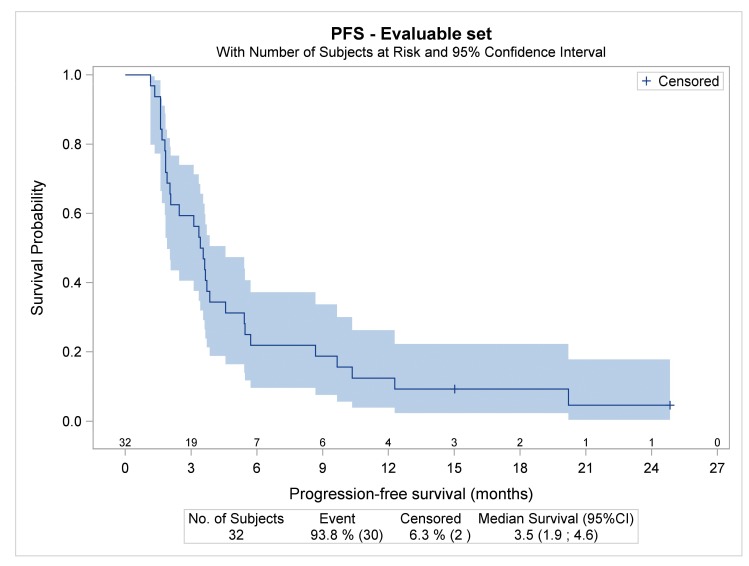
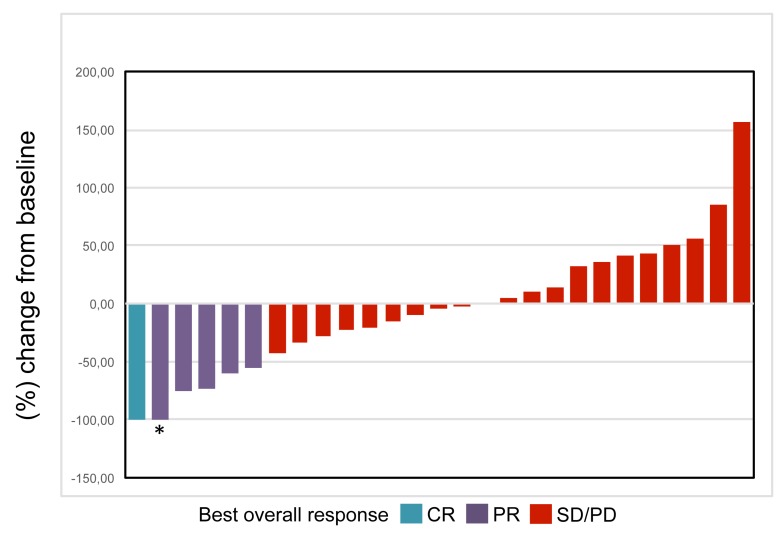
JAK2 constitutive activation/overexpression is common in classical Hodgkin lymphoma, and several cytokines stimulate Hodgkin lymphoma cells by recognizing JAK1-/JAK2-bound receptors. JAK blockade may thus be therapeutically beneficial in Hodgkin lymphoma. In this phase II study we assessed the safety and efficacy of ruxolitinib, an oral JAK1/2 inhibitor, in patients with relapsed/refractory Hodgkin lymphoma. The primary objective was overall response rate according to the International Harmonization Project 2007 criteria. Thirty-three patients with advanced disease (median number of prior lines of treatment: 5; refractory: 82%) were included; nine (27.3%) received at least six cycles of ruxolitinib and six (18.2%) received more than six cycles. The overall response rate after six cycles was 9.4% (3/32 patients). All three responders had partial responses; another 11 patients had transient stable disease. Best overall response rate was 18.8% (6/32 patients). Rapid alleviation of B-symptoms was common. The median duration of response was 7.7 months, median progression-free survival 3.5 months (95% CI: 1.9-4.6), and the median overall survival 27.1 months (95% CI: 14.4-27.1). Forty adverse events were reported in 14/33 patients (42.4%). One event led to treatment discontinuation, while 87.5% of patients recovered without sequelae. Twenty-five adverse events were grade 3 or higher. These events were mostly anemia (n=11), all considered related to ruxolitinib. Other main causes of grade 3 or higher adverse events included lymphopenia and infections. Of note, no cases of grade 4 neutropenia or thrombocytopenia were observed. Ruxolitinib shows signs of activity, albeit short-lived, beyond a simple anti-inflammatory effect. Its limited toxicity suggests that it has the potential to be combined with other therapeutic modalities. .
JAK2 组成性激活/过表达在经典霍奇金淋巴瘤中很常见,几种细胞因子通过识别 JAK1-/JAK2 结合受体刺激霍奇金淋巴瘤细胞。因此,JAK 阻断可能对霍奇金淋巴瘤具有治疗益处。在这项 2 期研究中,我们评估了口服 JAK1/2 抑制剂鲁索利替尼在复发/难治性霍奇金淋巴瘤患者中的安全性和疗效。主要终点是根据国际协调计划 2007 标准评估的总体缓解率。33 例晚期疾病患者(中位数治疗线数:5;难治性:82%)入选;9 例(27.3%)接受至少 6 个周期的鲁索利替尼治疗,6 例(18.2%)接受超过 6 个周期的治疗。6 个周期后的总体缓解率为 9.4%(32 例患者中的 3 例)。所有 3 例缓解者均有部分缓解;另外 11 例患者有短暂的稳定疾病。最佳总体缓解率为 18.8%(32 例患者中的 6 例)。快速缓解 B 症状很常见。缓解持续时间中位数为 7.7 个月,无进展生存期中位数为 3.5 个月(95%CI:1.9-4.6),总生存期中位数为 27.1 个月(95%CI:14.4-27.1)。33 例患者中有 14 例(42.4%)报告了 40 例不良事件。1 例不良事件导致治疗中断,而 87.5%的患者无后遗症恢复。25 例不良事件为 3 级或更高。这些事件主要为贫血(n=11),均认为与鲁索利替尼有关。其他 3 级或更高不良事件的主要原因包括淋巴细胞减少和感染。值得注意的是,未观察到 4 级中性粒细胞减少或血小板减少的情况。鲁索利替尼显示出活性迹象,尽管短暂,但超出了单纯的抗炎作用。其有限的毒性表明它有可能与其他治疗方式联合使用。