Qu Yusheng, Page Guy, Abi-Gerges Najah, Miller Paul E, Ghetti Andre, Vargas Hugo M
Integrated Discovery and Safety Pharmacology, Amgen Inc., Thousand Oaks, CA, United States.
AnaBios Corporation, San Diego, CA, United States.
Front Physiol. 2018 Jan 5;8:1109. doi: 10.3389/fphys.2017.01109. eCollection 2017.
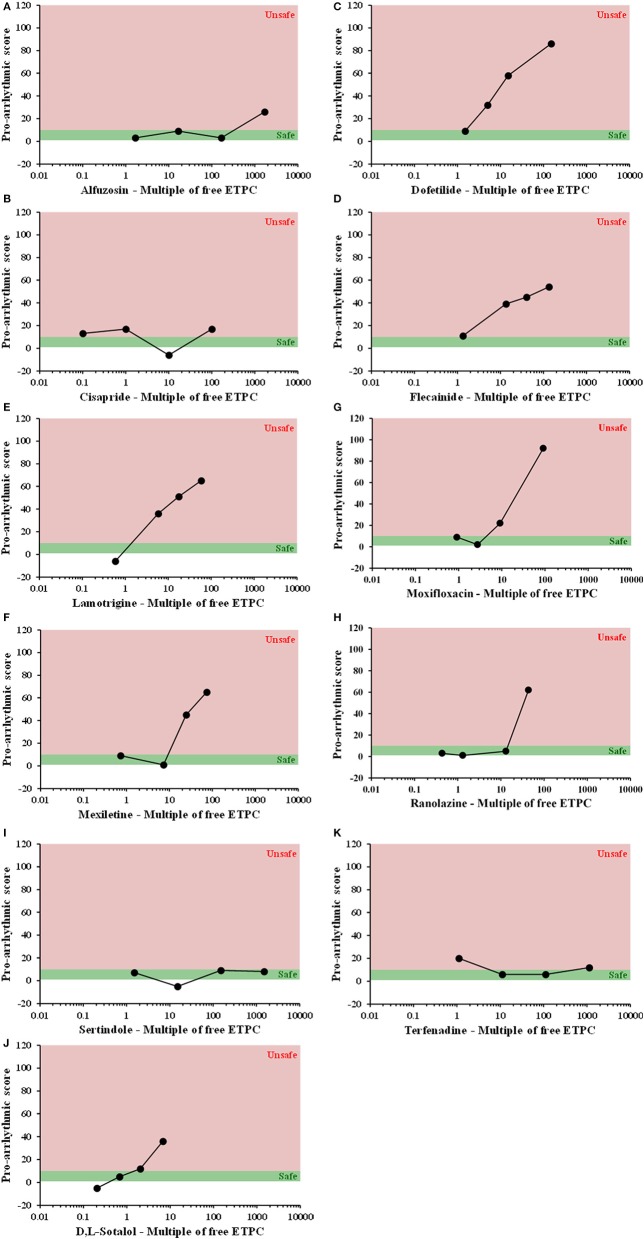
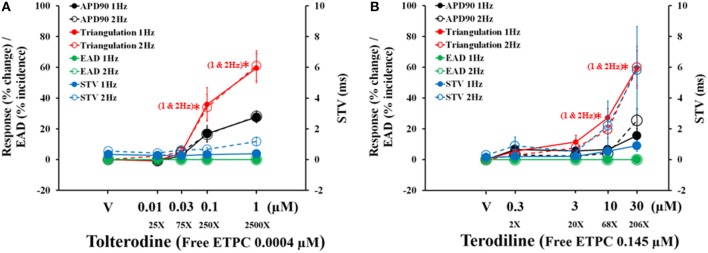
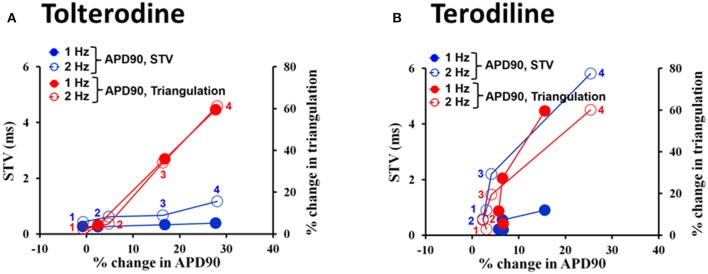
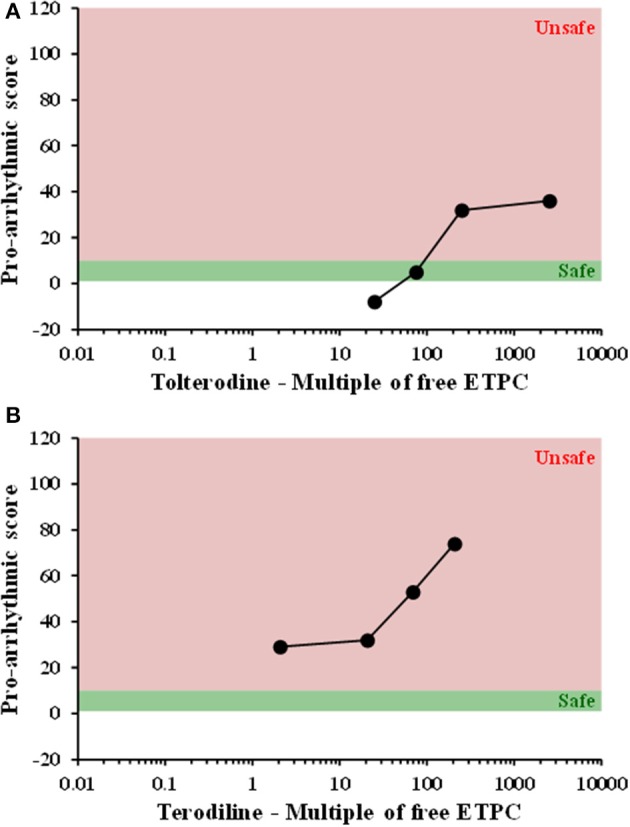
To assess drug-induced pro-arrhythmic risk, especially Torsades de Pointe (TdP), new models have been proposed, such as modeling of ventricular action potential (AP) and stem cell-derived cardiomyocytes (SC-CMs). Previously we evaluated the electrophysiological profile of 15 reference drugs in hESC-CMs and hiPSC-CMs for their effects on intracellular AP and extracellular field potential, respectively. Our findings indicated that SC-CMs exhibited immature phenotype and had the propensity to generate false positives in predicting TdP risk. To expand our knowledge with mature human cardiac tissues for drug-induced pro-arrhythmic risk assessment, human ventricular trabeculae (hVT) from ethically consented organ donors were used to evaluate the effects of the same 15 drugs (8 torsadogenic, 5 non-torsadogenic, and 2 discovery molecules) on AP parameters at 1 and 2 Hz. Each drug was tested blindly with 4 concentrations in duplicate trabeculae from 2 hearts. To identify the pro-arrhythmic risk of each drug, a pro-arrhythmic score was calculated as the weighted sum of percent drug-induced changes compared to baseline in various AP parameters, including AP duration and recognized pro-arrhythmia predictors such as triangulation, beat-to-beat variability and incidence of early-afterdepolarizations, at each concentration. In addition, to understand the translation of this preclinical hVT AP-based model to clinical studies, a ratio that relates each testing concentration to the human therapeutic unbound Cmax (Cmax) was calculated. At a ratio of 10, for the 8 torsadogenic drugs, 7 were correctly identified by the pro-arrhythmic score; 1 was mislabeled. For the 5 non-torsadogenic drugs, 4 were correctly identified as safe; 1 was mislabeled. Calculation of sensitivity, specificity, positive predictive value, and negative predictive value indicated excellent performance. For example, at a ratio of 10, scores for sensitivity, specificity, positive predictive value and negative predictive values were 0.88, 0.8, 0.88 and 0.8, respectively. Thus, the hVT AP-based model combined with the integrated analysis of pro-arrhythmic score can differentiate between torsadogenic and non-torsadogenic drugs, and has a greater predictive performance when compared to human SC-CM models.
为评估药物诱发的致心律失常风险,尤其是尖端扭转型室速(TdP),人们提出了一些新模型,如心室动作电位(AP)建模和干细胞衍生的心肌细胞(SC-CMs)。此前,我们分别评估了15种参考药物在人胚胎干细胞来源的心肌细胞(hESC-CMs)和人诱导多能干细胞来源的心肌细胞(hiPSC-CMs)中的电生理特征,以观察它们对细胞内AP和细胞外场电位的影响。我们的研究结果表明,SC-CMs表现出不成熟的表型,在预测TdP风险时容易产生假阳性。为了通过成熟的人体心脏组织扩展我们对药物诱发的致心律失常风险评估的认识,我们使用了来自符合伦理同意的器官捐献者的人室小梁(hVT)来评估相同的15种药物(8种致TdP药物、5种非致TdP药物和2种探索性分子)在1Hz和2Hz时对AP参数的影响。每种药物在来自2颗心脏的小梁中以4种浓度进行双份测试,测试时保持盲态。为了确定每种药物的致心律失常风险,计算了一个致心律失常评分,该评分是与基线相比,每种浓度下各种AP参数(包括AP持续时间以及公认的致心律失常预测指标,如三角化、逐搏变异性和早后去极化发生率)中药物诱发变化百分比的加权总和。此外,为了了解这种基于临床前hVT AP的模型在临床研究中的转化情况,计算了每个测试浓度与人体治疗性未结合Cmax(Cmax)的比值。在比值为10时,对于8种致TdP药物,致心律失常评分正确识别出了7种;1种被误判。对于5种非致TdP药物,4种被正确识别为安全;1种被误判。敏感性、特异性、阳性预测值和阴性预测值的计算表明该模型表现出色。例如,在比值为10时,敏感性、特异性、阳性预测值和阴性预测值的评分分别为0.88、0.8、0.88和0.8。因此,基于hVT AP的模型结合致心律失常评分的综合分析可以区分致TdP药物和非致TdP药物,并且与人体SC-CM模型相比具有更强的预测性能。