Xia Lei, Li Wen-Zheng, Liu Huan-Zhong, Hao Rui, Zhang Xiang-Yang
1 Department of Psychiatry, Chaohu Hospital of Anhui Medical University , Hefei, China .
2 Department of Psychiatry, Anhui Psychiatric Center, Anhui Medical University , Hefei, China .
J Child Adolesc Psychopharmacol. 2018 May;28(4):244-251. doi: 10.1089/cap.2017.0120. Epub 2018 Jan 22.
To compare the efficacy and safety of olanzapine and risperidone in children and adolescents (aged ≤18 years) with psychosis by conducting a meta-analysis of randomized controlled trials (RCTs).
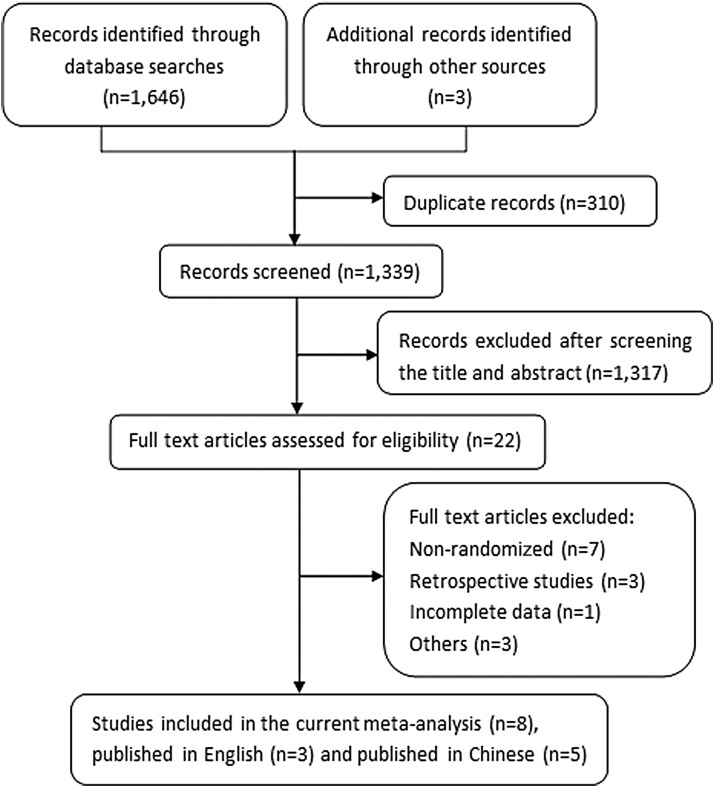
Several English and Chinese databases were searched for studies published before February 8th, 2017. Two independent investigators screened the studies according to prespecified criteria and extracted the data. Review Manager 5.3 was used to conduct the data synthesis.
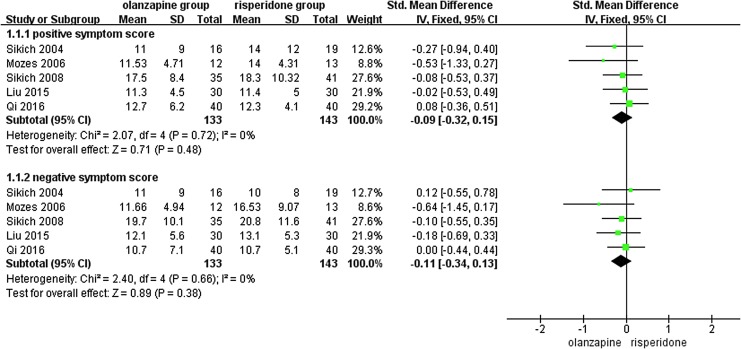
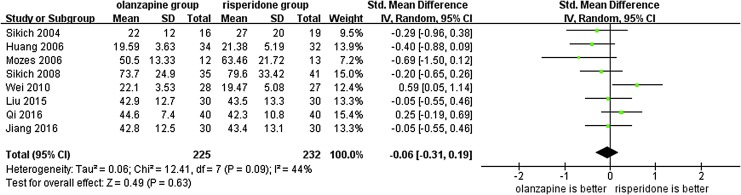
Eight RCTs involving 457 participants (225 participants in the olanzapine group and 232 participants in the risperidone group) were included. No significant differences were observed in the mean scores on the Positive and Negative Syndrome Scale/Brief Psychiatric Rating Scale (standard mean difference [SMD] = -0.06, 95% confidence intervals [CI] = [-0.31, 0.19], p = 0.63), the positive symptom scores (SMD = -0.09, 95% CI = [-0.32, 0.15], p = 0.48), or the negative symptom scores (SMD = -0.11 95% CI = [-0.34, 0.13], p = 0.38) between the two groups. Regarding adverse effects, the mean increases in weight (MD = 2.90, 95% CI = [1.41, 4.39], p = 0.0001), body mass index (MD = 0.90, 95% CI = [0.42, 1.38], p = 0.0003), and incidence of hypersomnia (risk ratios [RR] = 1.98, 95% CI = [1.15, 3.43], p = 0.01) were higher in the olanzapine group, while the incidence of insomnia (RR = 0.31, 95% CI = [0.11, 0.85], p = 0.02), prolactin elevation (RR = 0.11, 95% CI = [0.01, 0.85], p = 0.03), myotonia (RR = 0.12, 95% CI = [0.03, 0.49], p = 0.003), tremor (RR = 0.22, 95% CI = [0.08, 0.63], p = 0.005), and akathisia (RR = 0.27, 95% CI = [0.12, 0.57], p = 0.0007) was higher in the risperidone group.
There is no significant difference in efficacy between olanzapine and risperidone for the treatment of children and adolescents with psychosis, but the side effect profiles of these two medications differ. High-quality RCTs are needed before recommending clinical treatment in children and adolescents.
通过对随机对照试验(RCT)进行荟萃分析,比较奥氮平和利培酮治疗儿童及青少年(年龄≤18岁)精神病的疗效和安全性。
检索了几个英文和中文数据库,查找2017年2月8日前发表的研究。两名独立研究者根据预先设定的标准筛选研究并提取数据。使用Review Manager 5.3进行数据合成。
纳入了8项RCT,共457名参与者(奥氮平组225名参与者,利培酮组232名参与者)。两组在阳性和阴性症状量表/简明精神病评定量表上的平均得分(标准平均差[SMD]= -0.06,95%置信区间[CI]=[-0.31, 0.19],p = 0.63)、阳性症状得分(SMD = -0.09,95% CI = [-0.32, 0.15],p = 0.48)或阴性症状得分(SMD = -0.11,95% CI = [-0.34, 0.13],p = 0.38)方面均未观察到显著差异。在不良反应方面,奥氮平组体重平均增加量(MD = 2.90,95% CI = [1.41, 4.39],p = 0.0001)、体重指数(MD = 0.90,95% CI = [0.42, 1.38],p = 0.0003)以及嗜睡发生率(风险比[RR]= 1.98,95% CI = [1.15, 3.43],p = 0.01)更高,而利培酮组失眠发生率(RR = 0.31,95% CI = [0.11, 0.85],p = 0.02)、催乳素升高发生率(RR = 0.11,95% CI = [0.01, 0.85],p = 0.03)、肌强直发生率(RR = 0.12,95% CI = [0.03, 0.49],p = 0.003)、震颤发生率(RR = 0.22,95% CI = [0.08, 0.63],p = 0.005)和静坐不能发生率(RR = 0.27,95% CI = [0.12, 0.57],p = 0.0007)更高。
奥氮平和利培酮治疗儿童及青少年精神病的疗效无显著差异,但这两种药物的副作用情况不同。在推荐对儿童及青少年进行临床治疗之前,需要高质量的RCT。