Department of Orthopedic Trauma, Beijing Jishuitan Hospital, Beijing 100035, China.
Department of Hand Surgery, Beijing Jishuitan Hospital, Beijing 100035, China.
Chin Med J (Engl). 2018 Feb 5;131(3):282-288. doi: 10.4103/0366-6999.223851.
Surgical decompression of the ulnar nerve is effective for cubital tunnel syndrome. However, deep approaches may result in iatrogenic elbow stiffness. This long-term study was to evaluate the range of motion (ROM) of the elbow and functional outcomes after anterior subcutaneous transposition.
A total of 115 patients (78 male and 37 female; mean age: 46.6 years) who underwent anterior subcutaneous transposition of the ulnar nerve between 2001 and 2005 were evaluated retrospectively; mean follow-up was 13.5 years. Elbow ROM was measured as flexion arc, flexion, and extension preoperatively and at the final follow-up, and compared via a mixed analysis of variance adjusting for age. Neuropathy was assessed preoperatively using a modified McGowan neuropathy grade and postoperatively using modified Wilson-Krout criteria. An ordinal logistic regression analysis used postoperative modified Wilson-Krout criteria as the outcome and preoperative factors as predictors.
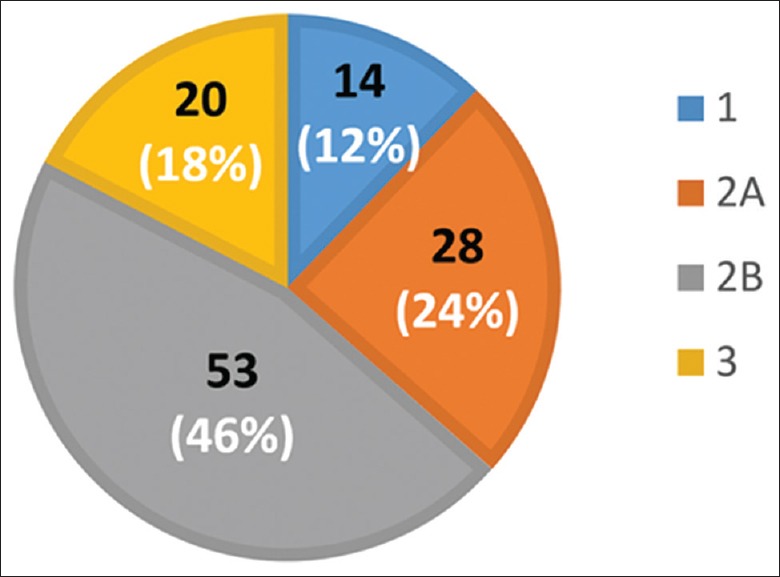
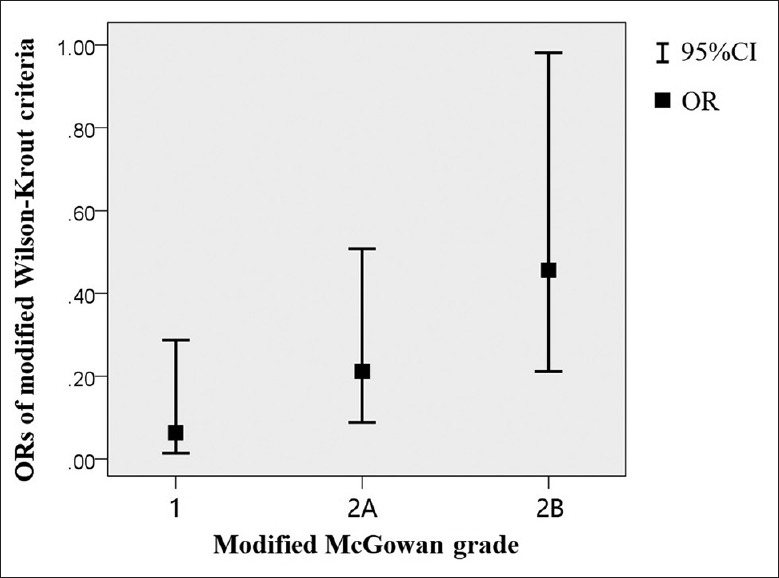
Preoperative McGowan grades were Grade 1 in 14 patients (12.2%), Grade 2A in 28 (24.3%), Grade 2B in 53 (46.1%), and Grade 3 in 20 (17.4%) patients. Postoperatively, 66 patients (57.4%) had excellent results, 26 (22.6%) had good results, 16 (13.9%) had fair results, and 7 (6.1%) had poor results at the final follow-up, as per the Wilson-Krout criteria. There were no complications. Pre- and postoperative elbow ROM was significantly decreased in patients with previous trauma or surgery of the elbow compared with those without (P < 0.05). Anterior subcutaneous transposition of the ulnar nerve did not significantly affect elbow ROM regardless of previous trauma or surgical history nor preoperative ROM (P > 0.05), after adjusting for age. Patients with prolonged symptoms prior to surgery and worse neuropathy tended to have less satisfactory functional outcomes (P < 0.05), after adjusting for covariates.
Anterior subcutaneous transposition of the ulnar nerve is an effective and reliable treatment of cubital tunnel syndrome with satisfactory outcomes and minimal effect on elbow ROM.
手术减压治疗肘管综合征有效,但深部入路可能导致医源性肘僵硬。本长期研究旨在评估肘前皮下尺神经前置术后的关节活动度(ROM)和功能结果。
回顾性分析 2001 年至 2005 年间行肘前皮下尺神经前置术的 115 例患者(78 例男性,37 例女性;平均年龄:46.6 岁);平均随访 13.5 年。测量术前和末次随访时的肘 ROM,包括屈弧、屈肘和伸肘,并通过混合方差分析进行比较,调整年龄因素。术前采用改良 McGowan 神经病学分级评估神经病,术后采用改良 Wilson-Krout 标准评估。采用术后改良 Wilson-Krout 标准作为结果,术前因素作为预测因子的有序逻辑回归分析。
术前 McGowan 分级为 1 级 14 例(12.2%),2A 级 28 例(24.3%),2B 级 53 例(46.1%),3 级 20 例(17.4%)。术后 Wilson-Krout 标准评定,66 例(57.4%)优,26 例(22.6%)良,16 例(13.9%)可,7 例(6.1%)差。无并发症。与无肘部既往创伤或手术史者相比,有肘部既往创伤或手术史者术前及术后的肘 ROM 显著降低(P < 0.05)。无论是否有肘部既往创伤或手术史,也无论术前 ROM 如何,尺神经肘前皮下前置术对肘部 ROM 均无显著影响(P > 0.05),校正年龄后。术前症状持续时间较长和神经病变较严重的患者功能结局较差(P < 0.05),校正协变量后。
肘前皮下尺神经前置术是治疗肘管综合征的一种有效、可靠的方法,其结果满意,对肘部 ROM 的影响最小。