Hayes Aimee R, Brungs Daniel, Pavlakis Nick
Department of Medical Oncology, Royal North Shore Hospital, St Leonards, New South Wales, Australia.
Department of Medical Oncology, Illawarra Cancer Care Centre, Wollongong Hospital, Wollongong, New South Wales, Australia.
PLoS One. 2018 Jan 25;13(1):e0191455. doi: 10.1371/journal.pone.0191455. eCollection 2018.
In advanced prostate cancer, osteoclast inhibitors prevent and palliate skeletal related events associated with bone metastases. However, it is uncertain whether they play a disease-modifying role earlier in the course of the disease.
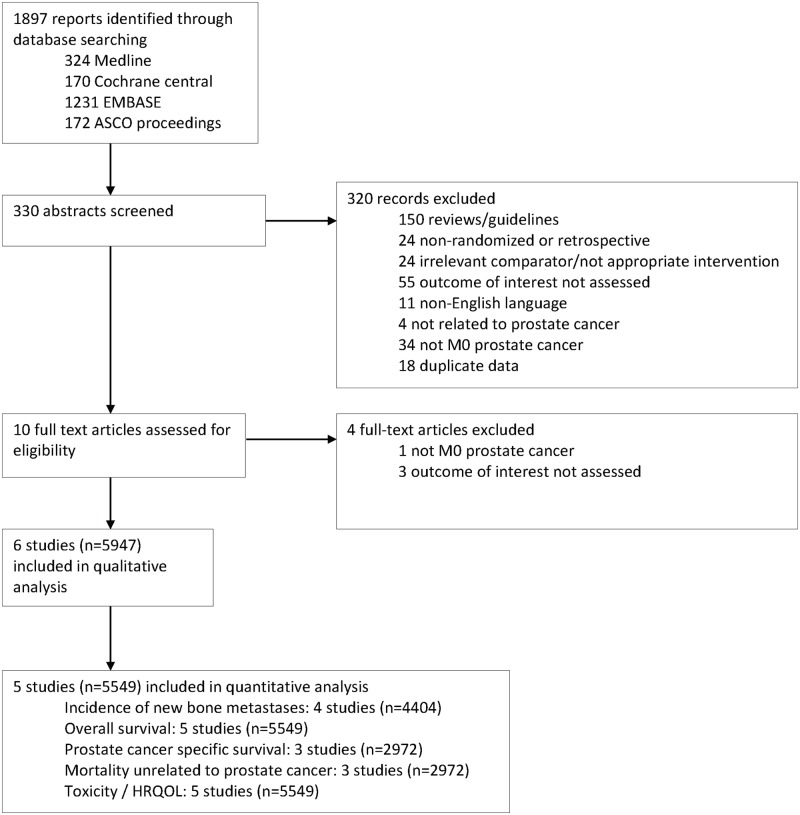
Medline, EMBASE, Cochrane Central Register of Controlled Trials and Cochrane Database of Systematic Reviews and ASCO conference proceedings were searched for randomized controlled trials that compared osteoclast inhibitors with placebo and/or standard of care (SOC) in patients with high-risk, non-metastatic prostate cancer. The primary outcome measure was incidence of new bone metastases; secondary outcomes included overall survival (OS), prostate cancer specific survival, mortality unrelated to prostate cancer, toxicity and health related quality of life outcomes. Results are presented as relative risk (RR) with 95% confidence intervals (CI).
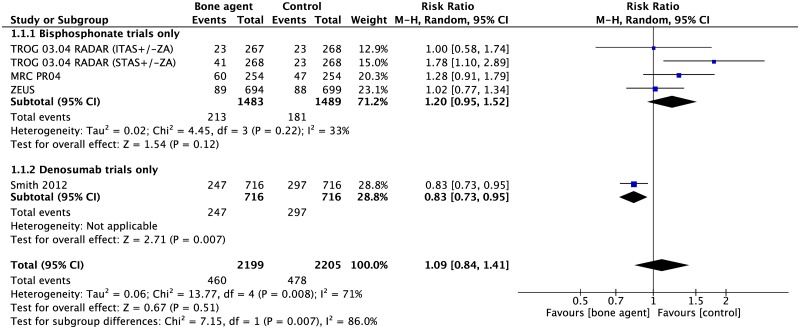
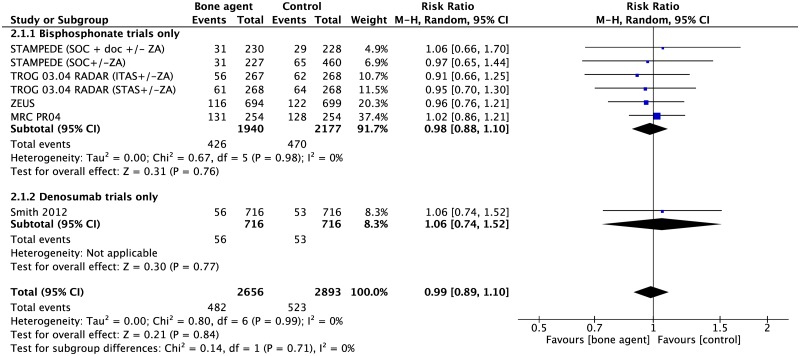
Six randomized controlled trials (5947 participants) were included, five evaluating bisphosphonates and one denosumab. Overall, there was no difference in incidence of bone metastases between participants treated with osteoclast inhibitors versus placebo/SOC (RR 1.09, 95%CI 0.84-1.41, p = 0.51) however significant heterogeneity was observed between studies. The denosumab trial was the largest and only positive trial amongst the included studies (RR 0.83, 95%CI 0.73-0.95, p = 0.007). No significant difference was observed in OS (RR 0.99 95% CI 0.89-1.10, p = 0.84) nor prostate cancer specific survival (RR 1.12 95%CI 0.93-1.36, p = 0.24). Most studies reported increased rates of osteonecrosis of the jaw (5% or less) and hypocalcemia (2% or less) with osteoclast inhibitors.
While there is limited evidence that bisphosphonates alter the natural history of high-risk, non-metastatic prostate cancer, denosumab delays onset of bone metastases in this patient population. Neither class of osteoclast inhibitor demonstrated an impact on survival outcomes. Future trials with better defined patient selection and a robust definition for high risk disease is critical.
在晚期前列腺癌中,破骨细胞抑制剂可预防和缓解与骨转移相关的骨相关事件。然而,它们在疾病进程早期是否发挥疾病修饰作用尚不确定。
检索Medline、EMBASE、Cochrane对照试验中心注册库、Cochrane系统评价数据库和美国临床肿瘤学会会议论文集,查找在高危、非转移性前列腺癌患者中比较破骨细胞抑制剂与安慰剂和/或标准治疗(SOC)的随机对照试验。主要结局指标是新发骨转移的发生率;次要结局包括总生存期(OS)、前列腺癌特异性生存期、与前列腺癌无关的死亡率、毒性和健康相关生活质量结局。结果以相对风险(RR)及95%置信区间(CI)表示。
纳入6项随机对照试验(5947名参与者),5项评估双膦酸盐,1项评估地诺单抗。总体而言,接受破骨细胞抑制剂治疗的参与者与接受安慰剂/SOC治疗的参与者相比,骨转移发生率无差异(RR 1.09,95%CI 0.84 - 1.41,p = 0.51),但各研究间观察到显著异质性。地诺单抗试验是纳入研究中规模最大且唯一呈阳性结果的试验(RR 0.83,95%CI 0.73 - 0.95,p = 0.007)。在OS(RR 0.99,95%CI 0.89 - 1.10,p = 0.84)和前列腺癌特异性生存期方面均未观察到显著差异(RR 1.12,95%CI 0.93 - 1.36,p = 0.24)。大多数研究报告使用破骨细胞抑制剂时颌骨坏死(5%或更低)和低钙血症(2%或更低)的发生率增加。
虽然仅有有限证据表明双膦酸盐可改变高危、非转移性前列腺癌的自然病程,但地诺单抗可延缓该患者群体骨转移的发生。两类破骨细胞抑制剂均未显示对生存结局有影响。未来进行更明确的患者选择和对高危疾病进行更可靠定义的试验至关重要。