Department of Vascular and Endovascular Surgery, Heinrich-Heine-University Medical Center Düsseldorf, 40225 Düsseldorf, Germany.
Department for Vascular and Endovascular Surgery, Klinikum Rechts der Isar Technical University, 81675 Munich, Germany.
Int J Mol Sci. 2018 Jan 26;19(2):374. doi: 10.3390/ijms19020374.
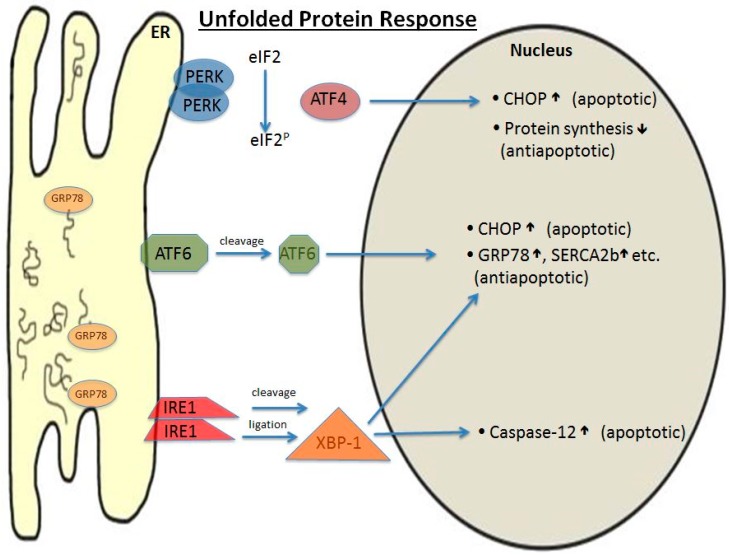
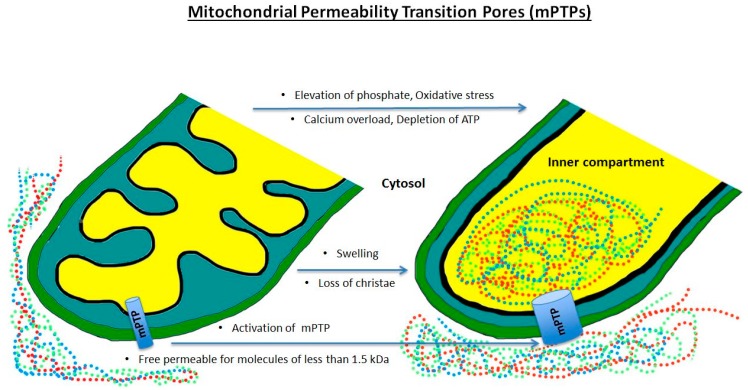
Acute ischemia of an extremity occurs in several stages, a lack of oxygen being the primary contributor of the event. Although underlying patho-mechanisms are similar, it is important to determine whether it is an acute or chronic event. Healthy tissue does not contain enlarged collaterals, which are formed in chronically malperfused tissue and can maintain a minimum supply despite occlusion. The underlying processes for enhanced collateral blood flow are sprouting vessels from pre-existing vessels (via angiogenesis) and a lumen extension of arterioles (via arteriogenesis). While disturbed flow patterns with associated local low shear stress upregulate angiogenesis promoting genes, elevated shear stress may trigger arteriogenesis due to increased blood volume. In case of an acute ischemia, especially during the reperfusion phase, fluid transfer occurs into the tissue while the vascular bed is simultaneously reduced and no longer reacts to vaso-relaxing factors such as nitric oxide. This process results in an exacerbative cycle, in which increased peripheral resistance leads to an additional lack of oxygen. This whole process is accompanied by an inundation of inflammatory cells, which amplify the inflammatory response by cytokine release. However, an extremity is an individual-specific composition of different tissues, so these processes may vary dramatically between patients. The image is more uniform when broken down to the single cell stage. Because each cell is dependent on energy produced from aerobic respiration, an event of acute hypoxia can be a life-threatening situation. Aerobic processes responsible for yielding adenosine triphosphate (ATP), such as the electron transport chain and oxidative phosphorylation in the mitochondria, suffer first, thus disrupting the integrity of cellular respiration. One consequence of this is irreparable damage of the cell membrane due to an imbalance of electrolytes. The eventual increase in net fluid influx associated with a decrease in intracellular pH is considered an end-stage event. Due to the lack of ATP, individual cell organelles can no longer sustain their activity, thus initiating the cascade pathways of apoptosis via the release of cytokines such as the BCL2 associated X protein (BAX). As ischemia may lead to direct necrosis, inflammatory processes are further aggravated. In the case of reperfusion, the flow of nascent oxygen will cause additional damage to the cell, further initiating apoptosis in additional surrounding cells. In particular, free oxygen radicals are formed, causing severe damage to cell membranes and desoxyribonucleic acid (DNA). However, the increased tissue stress caused by this process may be transient, as radical scavengers may attenuate the damage. Taking the above into final consideration, it is clearly elucidated that acute ischemia and subsequent reperfusion is a process that leads to acute tissue damage combined with end-organ loss of function, a condition that is difficult to counteract.
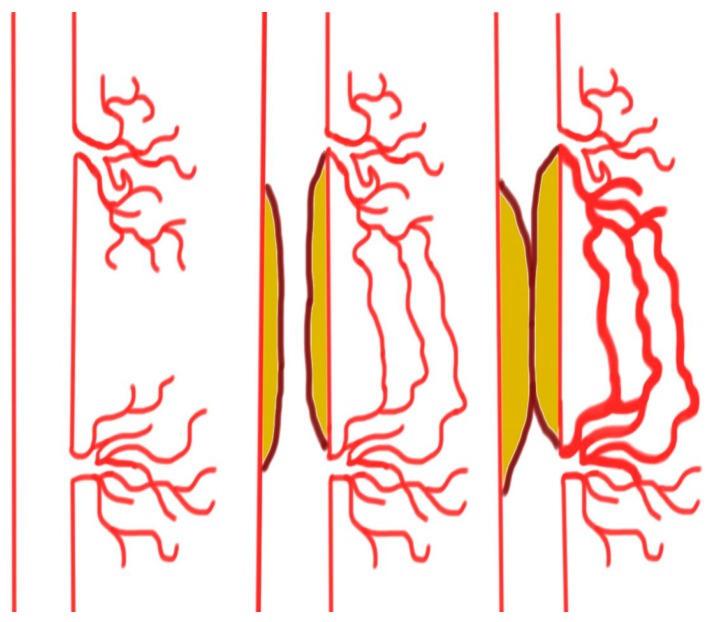
肢体急性缺血可分为几个阶段,其中缺氧是主要原因。尽管潜在的病理机制相似,但确定是急性还是慢性事件很重要。健康组织不含扩大的侧支循环,侧支循环在慢性灌注不良的组织中形成,即使发生阻塞也能维持最小的供应。增强侧支血流的潜在过程是通过血管生成从预先存在的血管中形成发芽血管(通过血管生成)和通过血管生成(通过血管生成)延伸小动脉的管腔。虽然与局部低剪切应力相关的紊乱血流模式上调促进血管生成的基因,但由于血流量增加,升高的剪切应力可能触发血管生成。在急性缺血的情况下,特别是在再灌注阶段,液体转移到组织中,同时血管床同时减少,并且不再对血管舒张因子(如一氧化氮)作出反应。这个过程导致一个恶化的循环,其中外周阻力增加导致进一步缺氧。这个过程伴随着炎症细胞的大量涌入,炎症细胞通过细胞因子的释放放大炎症反应。然而,肢体是由不同组织组成的个体特有的组成,因此这些过程在患者之间可能有很大的差异。当分解到单细胞阶段时,图像更加统一。因为每个细胞都依赖于有氧呼吸产生的能量,所以急性缺氧事件可能是危及生命的情况。负责产生三磷酸腺苷 (ATP) 的有氧过程,例如电子传递链和线粒体中的氧化磷酸化,首先受到影响,从而破坏细胞呼吸的完整性。其结果之一是由于电解质失衡导致细胞膜不可逆转的损伤。与细胞内 pH 值降低相关的净流体流入量的最终增加被认为是终末期事件。由于缺乏 ATP,单个细胞细胞器无法再维持其活性,从而通过释放细胞因子(如 BCL2 相关 X 蛋白(BAX))引发细胞凋亡级联途径。由于缺血可能导致直接坏死,炎症过程进一步加剧。在再灌注的情况下,新生氧的流动会对细胞造成额外的损伤,进一步引发周围细胞的凋亡。特别是,形成了自由基,对细胞膜和脱氧核糖核酸(DNA)造成严重损伤。然而,由于自由基清除剂可能减轻损伤,因此由该过程引起的组织压力增加可能是短暂的。综上所述,很明显,急性缺血和随后的再灌注是导致急性组织损伤和终末器官功能丧失的过程,这种情况很难逆转。