MRC Clinical Trials Unit, University College London (UCL), London, United Kingdom.
Institut National d'Etude Demographique (INED), Mortality, Health and Epidemiology Unit, Paris, France.
PLoS Med. 2018 Jan 30;15(1):e1002491. doi: 10.1371/journal.pmed.1002491. eCollection 2018 Jan.
Published estimates of mortality and progression to AIDS as children with HIV approach adulthood are limited. We describe rates and risk factors for death and AIDS-defining events in children and adolescents after initiation of combination antiretroviral therapy (cART) in 17 middle- and high-income countries, including some in Western and Central Europe (W&CE), Eastern Europe (Russia and Ukraine), and Thailand.
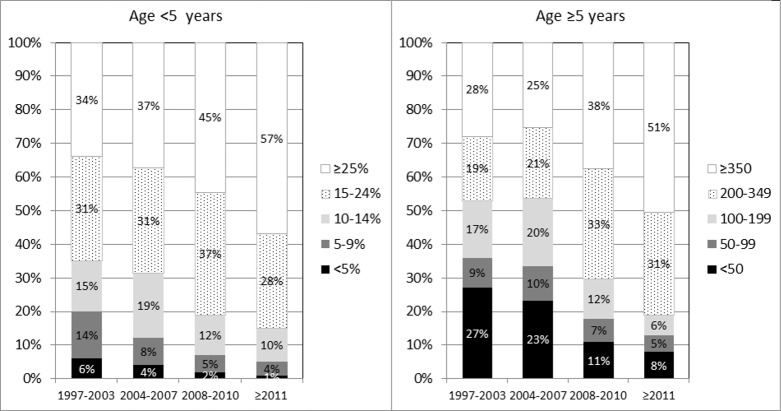
Children with perinatal HIV aged <18 years initiating cART were followed until their 21st birthday, transfer to adult care, death, loss to follow-up, or last visit up until 31 December 2013. Rates of death and first AIDS-defining events were calculated. Baseline and time-updated risk factors for early/late (≤/>6 months of cART) death and progression to AIDS were assessed. Of 3,526 children included, 32% were from the United Kingdom or Ireland, 30% from elsewhere in W&CE, 18% from Russia or Ukraine, and 20% from Thailand. At cART initiation, median age was 5.2 (IQR 1.4-9.3) years; 35% of children aged <5 years had a CD4 lymphocyte percentage <15% in 1997-2003, which fell to 15% of children in 2011 onwards (p < 0.001). Similarly, 53% and 18% of children ≥5 years had a CD4 count <200 cells/mm3 in 1997-2003 and in 2011 onwards, respectively (p < 0.001). Median follow-up was 5.6 (2.9-8.7) years. Of 94 deaths and 237 first AIDS-defining events, 43 (46%) and 100 (42%) were within 6 months of initiating cART, respectively. Multivariable predictors of early death were: being in the first year of life; residence in Russia, Ukraine, or Thailand; AIDS at cART start; initiating cART on a nonnucleoside reverse transcriptase inhibitor (NNRTI)-based regimen; severe immune suppression; and low BMI-for-age z-score. Current severe immune suppression, low current BMI-for-age z-score, and current viral load >400 c/mL predicted late death. Predictors of early and late progression to AIDS were similar. Study limitations include incomplete recording of US Centers for Disease Control (CDC) disease stage B events and serious adverse events in some countries; events that were distributed over a long time period, and that we lacked power to analyse trends in patterns and causes of death over time.
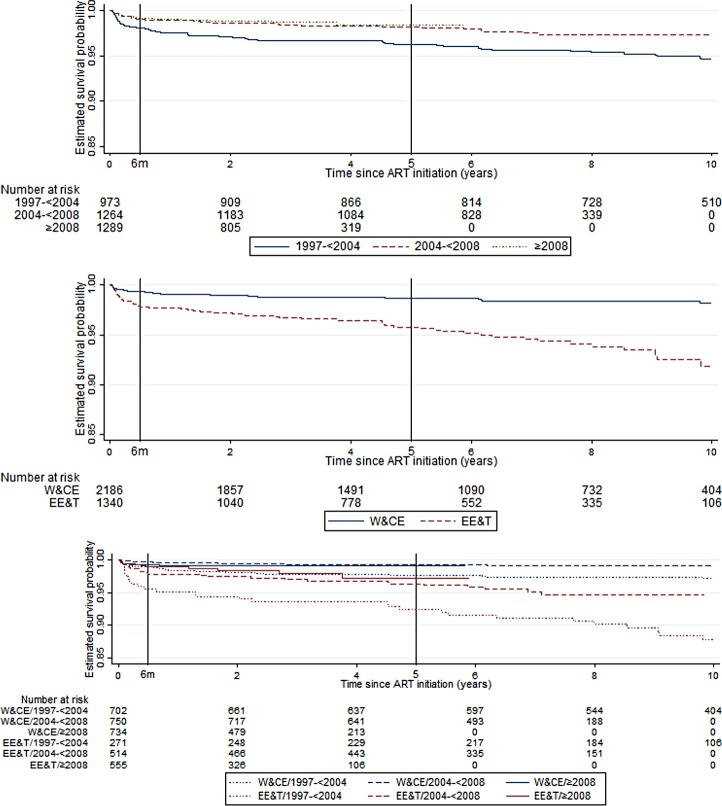
In our study, 3,526 children and adolescents with perinatal HIV infection initiated antiretroviral therapy (ART) in countries in Europe and Thailand. We observed that over 40% of deaths occurred ≤6 months after cART initiation. Greater early mortality risk in infants, as compared to older children, and in Russia, Ukraine, or Thailand as compared to W&CE, raises concern. Current severe immune suppression, being underweight, and unsuppressed viral load were associated with a higher risk of death at >6 months after initiation of cART.
目前有关接近成年的 HIV 感染儿童死亡率和艾滋病进展的发表数据十分有限。我们描述了在 17 个中高收入国家(包括一些西欧和中欧、东欧(俄罗斯和乌克兰)以及泰国)启动联合抗逆转录病毒治疗(cART)后,儿童和青少年的死亡率和艾滋病定义事件的发生率和风险因素。
年龄小于 18 岁、经围生期感染 HIV 的儿童在开始 cART 后,直至 21 岁生日、转至成人护理、死亡、失访或截至 2013 年 12 月 31 日的最后一次就诊时,一直进行随访。计算死亡率和首次艾滋病定义事件的发生率。评估了早期/晚期(≤6 个月 cART)死亡和艾滋病进展的基线和时间更新风险因素。在纳入的 3526 名儿童中,32%来自英国或爱尔兰,30%来自西欧和中欧其他地区,18%来自俄罗斯或乌克兰,20%来自泰国。在 cART 开始时,中位年龄为 5.2(IQR 1.4-9.3)岁;在 1997-2003 年,有 35%的年龄<5 岁的儿童的 CD4 淋巴细胞百分比<15%,这一比例在 2011 年及以后下降至 15%(p<0.001)。同样,在 1997-2003 年和 2011 年及以后,分别有 53%和 18%的年龄≥5 岁的儿童的 CD4 计数<200 个细胞/mm3(p<0.001)。中位随访时间为 5.6(2.9-8.7)年。在 94 例死亡和 237 例首次艾滋病定义事件中,分别有 43(46%)和 100(42%)例发生在启动 cART 的 6 个月内。早期死亡的多变量预测因素为:生命的第一年;居住在俄罗斯、乌克兰或泰国;cART 开始时患有艾滋病;开始基于非核苷类逆转录酶抑制剂(NNRTI)的方案;严重免疫抑制;以及低体重指数年龄 Z 评分。目前严重的免疫抑制、目前低体重指数年龄 Z 评分和目前病毒载量>400 c/mL 预测晚期死亡。早期和晚期艾滋病进展的预测因素相似。研究的局限性包括美国疾病控制与预防中心(CDC)疾病阶段 B 事件和一些国家严重不良事件记录不完整;事件分布在很长一段时间内,我们没有足够的能力分析随时间推移而发生的死亡模式和原因的趋势。
在我们的研究中,3526 名患有围生期 HIV 感染的儿童和青少年在欧洲和泰国的国家开始接受抗逆转录病毒治疗(ART)。我们观察到,超过 40%的死亡发生在 cART 启动后 6 个月内。与大龄儿童相比,婴儿的早期死亡率更高,与西欧和中欧相比,俄罗斯、乌克兰或泰国的死亡率更高,这令人担忧。目前严重的免疫抑制、体重不足和未抑制的病毒载量与 cART 启动后>6 个月的死亡风险增加有关。