Huemer Florian, Weiss Lukas, Faber Viktoria, Neureiter Daniel, Egle Alexander, Geissler Klaus, Voskova Daniela, Zebisch Armin, Burgstaller Sonja, Pichler Angelika, Stauder Reinhard, Sperr Wolfgang, Lang Alois, Pfeilstöcker Michael, Machherndl-Spandl Sigrid, Stampfl Margarete, Greil Richard, Pleyer Lisa
Department of Internal Medicine III with Hematology, Medical Oncology, Hemostaseology, Infectious Disease, Rheumatology, Oncologic Center, Laboratory of Immunological and Molecular Cancer Research, Paracelsus Medical University Salzburg, Muellner Hauptstraße 48, 5020, Salzburg, Austria.
Cancer Cluster Salzburg, Salzburg, Austria.
Wien Klin Wochenschr. 2018 Feb;130(3-4):115-125. doi: 10.1007/s00508-018-1315-2. Epub 2018 Jan 30.
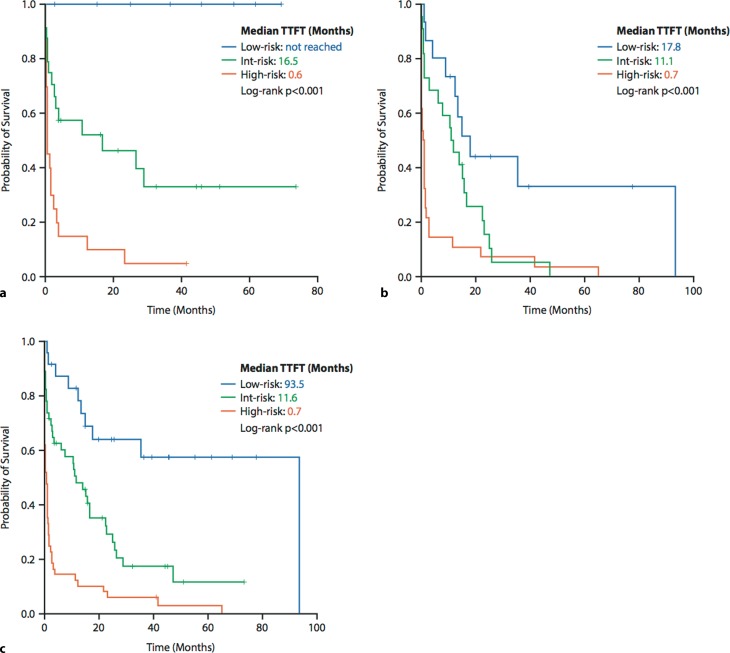
Chronic myelomonocytic leukaemia is a rare disease and data on the treatment are often extrapolated from myelodysplastic syndrome studies. Although several scores exist for the prognosis of overall survival in chronic myelomonocytic leukaemia, so far there is no designated score for the prediction of the time to first treatment. We tested clinical parameters and cytogenetic information for their ability to predict the time to first treatment in our single center cohort of 55 unselected consecutive chronic myelomonocytic leukaemia patients. In multivariate analysis we identified elevated lactate dehydrogenase (≥223 U/l), higher bone marrow blast percentage (≥7.5%) and thrombocytopenia (<55 G/l) at initial diagnosis as the most relevant parameters for the time to first treatment. Using these three parameters we developed a risk score that efficiently estimates the time to treatment initiation with azacitidine or hydroxyurea (p < 0.001; log-rank). In the high-risk group (≥2 risk factors) 85% of patients required treatment within 1 year, whereas this was the case in 48% in the intermediate-risk (1 risk factor) and in 0% in the low-risk group (0 risk factors). Our risk model was validated in an external test cohort of 65 patients and may serve as a simplified and easily applicable tool for identifying patients who may not require early treatment initiation.
慢性粒单核细胞白血病是一种罕见疾病,有关其治疗的数据通常是从骨髓增生异常综合征研究中推断出来的。尽管存在多种用于预测慢性粒单核细胞白血病总生存预后的评分,但到目前为止,尚无专门用于预测首次治疗时间的评分。我们在由55例未经选择的连续慢性粒单核细胞白血病患者组成的单中心队列中,测试了临床参数和细胞遗传学信息预测首次治疗时间的能力。在多变量分析中,我们确定初诊时乳酸脱氢酶升高(≥223 U/l)、骨髓原始细胞百分比更高(≥7.5%)和血小板减少(<55 G/l)是首次治疗时间最相关的参数。利用这三个参数,我们制定了一个风险评分,可有效估计开始使用阿扎胞苷或羟基脲治疗的时间(p < 0.001;对数秩检验)。在高风险组(≥2个风险因素)中,85%的患者在1年内需要治疗,而中风险组(1个风险因素)为48%,低风险组(0个风险因素)为0%。我们的风险模型在一个由65例患者组成的外部测试队列中得到验证,可作为一种简单且易于应用的工具,用于识别可能不需要早期开始治疗的患者。