Morgan Nadia D, Shah Ami A, Mayes Maureen D, Domsic Robyn T, Medsger Thomas A, Steen Virginia D, Varga John, Carns Mary, Ramos Paula S, Silver Richard M, Schiopu Elena, Khanna Dinesh, Hsu Vivien, Gordon Jessica K, Gladue Heather, Saketkoo Lesley A, Criswell Lindsey A, Derk Chris T, Trojanowski Marcin A, Shanmugam Victoria K, Chung Lorinda, Valenzuela Antonia, Jan Reem, Goldberg Avram, Remmers Elaine F, Kastner Daniel L, Wigley Fredrick M, Gourh Pravitt, Boin Francesco
Division of Rheumatology, Johns Hopkins University School of Medicine, Baltimore, MD Division of Rheumatology, University of Texas-McGovern Medical School, Houston, TX Division of Rheumatology, University of Pittsburgh, PA Division of Rheumatology, Georgetown University School of Medicine, Washington, DC Division of Rheumatology, Northwestern University, Feinberg School of Medicine, Chicago, IL Division of Rheumatology, Medical University of South Carolina, Charleston, SC Division of Rheumatology, University of Michigan, Ann Arbor, MI Division of Rheumatology, Robert Wood Johnson University, New Brunswick, NJ Division of Rheumatology, Hospital for Special Surgery, New York, NY Department of Rheumatology, Arthritis and Osteoporosis Consultants of the Carolinas, Charlotte, NC Division of Rheumatology, Tulane University School of Medicine, New Orleans, LA Division of Rheumatology, University of California San Francisco, CA Division of Rheumatology, University of Pennsylvania, Philadelphia, PA Division of Rheumatology, Boston University School of Medicine, Boston, MA Division of Rheumatology, George Washington University, Washington, DC Division of Rheumatology, Stanford University School of Medicine, Stanford, CA Division of Rheumatology, University of Chicago Pritzker School of Medicine, Chicago, IL Division of Rheumatology, New York University Langone Medical Center, New York, NY National Human Genome Research Institute National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health, Bethesda, MD, USA.
Medicine (Baltimore). 2017 Dec;96(51):e8980. doi: 10.1097/MD.0000000000008980.
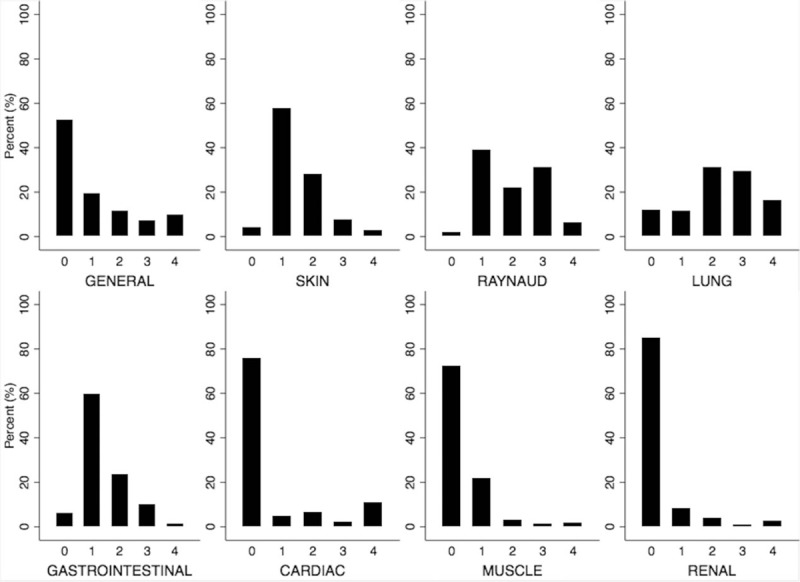
Racial differences exist in the severity of systemic sclerosis (SSc). To enhance our knowledge about SSc in African Americans, we established a comprehensive clinical database from the largest multicenter cohort of African American SSc patients assembled to date (the Genome Research in African American Scleroderma Patients (GRASP) cohort).African American SSc patients were enrolled retrospectively and prospectively over a 30-year period (1987-2016), from 18 academic centers throughout the United States. The cross-sectional prevalence of sociodemographic, clinical, and serological features was evaluated. Factors associated with clinically significant manifestations of SSc were assessed using multivariate logistic regression analyses.The study population included a total of 1009 African American SSc patients, comprised of 84% women. In total, 945 (94%) patients met the 2013 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for SSc, with the remaining 64 (6%) meeting the 1980 ACR or CREST (calcinosis, Raynaud's phenomenon, esophageal dysmotility, sclerodactyly, telangiectasia) criteria. While 43% were actively employed, 33% required disability support. The majority (57%) had the more severe diffuse subtype and a young age at symptom onset (39.1 ± 13.7 years), in marked contrast to that reported in cohorts of predominantly European ancestry. Also, 1 in 10 patients had a severe Medsger cardiac score of 4. Pulmonary fibrosis evident on computed tomography (CT) chest was present in 43% of patients and was significantly associated with anti-topoisomerase I positivity. 38% of patients with CT evidence of pulmonary fibrosis had a severe restrictive ventilator defect, forced vital capacity (FVC) ≤50% predicted. A significant association was noted between longer disease duration and higher odds of pulmonary hypertension, telangiectasia, and calcinosis. The prevalence of potentially fatal scleroderma renal crisis was 7%, 3.5 times higher than the 2% prevalence reported in the European League Against Rheumatism Scleroderma Trials and Research (EUSTAR) cohort.Our study emphasizes the unique and severe disease burden of SSc in African Americans compared to those of European ancestry.
系统性硬化症(SSc)的严重程度存在种族差异。为了增进我们对非裔美国人系统性硬化症的了解,我们从迄今为止组建的最大的非裔美国人系统性硬化症患者多中心队列(非裔美国硬皮病患者基因组研究(GRASP)队列)中建立了一个综合临床数据库。在30年期间(1987 - 2016年),从美国各地的18个学术中心对非裔美国人系统性硬化症患者进行了回顾性和前瞻性登记。评估了社会人口统计学、临床和血清学特征的横断面患病率。使用多变量逻辑回归分析评估与系统性硬化症临床显著表现相关的因素。研究人群总共包括1009名非裔美国人系统性硬化症患者,其中84%为女性。总共有945名(94%)患者符合2013年美国风湿病学会/欧洲抗风湿病联盟(ACR/EULAR)系统性硬化症分类标准,其余64名(6%)符合1980年ACR或CREST(钙质沉着、雷诺现象、食管动力障碍、指端硬化、毛细血管扩张)标准。虽然43%的患者积极就业,但33%的患者需要残疾支持。大多数(57%)患者患有更严重的弥漫性亚型,且症状发作时年龄较轻(39.1±13.7岁),这与主要为欧洲血统的队列报告形成明显对比。此外,十分之一的患者有严重的梅兹格心脏评分4分。胸部计算机断层扫描(CT)显示43%的患者存在肺纤维化,且与抗拓扑异构酶I阳性显著相关。有CT证据显示肺纤维化的患者中,38%有严重的限制性通气缺陷,用力肺活量(FVC)≤预测值的50%。病程较长与肺动脉高压、毛细血管扩张和钙质沉着的较高几率之间存在显著关联。潜在致命的硬皮病肾危象患病率为7%,比欧洲抗风湿病联盟硬皮病试验和研究(EUSTAR)队列报告的2%患病率高3.5倍。我们的研究强调了与欧洲血统患者相比,非裔美国人系统性硬化症独特且严重的疾病负担。