Department of Biostatistics, University of Kansas Medical Center, Kansas City, KS, USA.
Department of Neurology, University of Kansas Medical Center, Kansas City, KS, USA.
BMC Med Res Methodol. 2018 Feb 6;18(1):19. doi: 10.1186/s12874-018-0479-9.
Amyotrophic Lateral Sclerosis (ALS), also known as Lou Gehrig's disease, is a rare disease with extreme between-subject variability, especially with respect to rate of disease progression. This makes modelling a subject's disease progression, which is measured by the ALS Functional Rating Scale (ALSFRS), very difficult. Consider the problem of predicting a subject's ALSFRS score at 9 or 12 months after a given time-point.
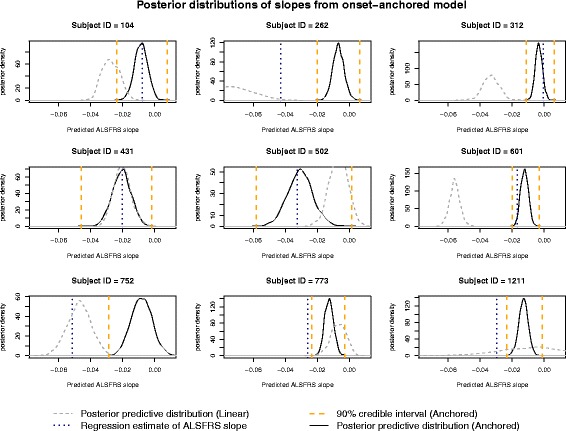
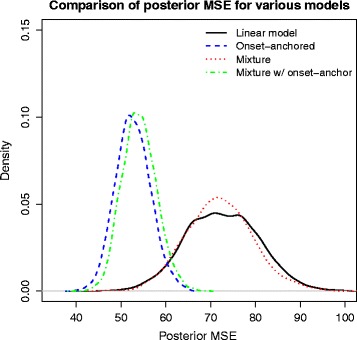
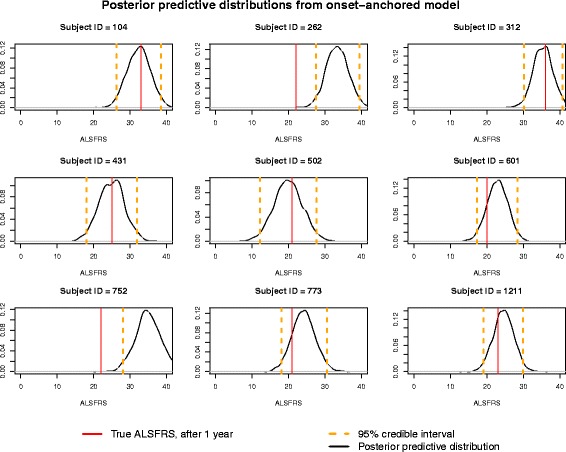
We obtained ALS subject data from the Pooled Resource Open-Access ALS Clinical Trials Database, a collection of data from various ALS clinical trials. Due to the typical linearity of the ALSFRS, we consider several Bayesian hierarchical linear models. These include a mixture model (to account for the two potential classes of "fast" and "slow" ALS progressors) as well as an onset-anchored model, in which an additional artificial data-point, using time of disease onset, is utilized to improve predictive performance.
The onset-anchored model had a drastically reduced posterior predictive mean-square-error distributions, when compared to the Bayesian hierarchical linear model or the mixture model under a cross-validation approach. No covariates, other than time of disease onset, consistently improved predictive performance in either the Bayesian hierarchical linear model or the onset-anchored model.
Augmenting patient data with an additional artificial data-point, or onset anchor, can drastically improve predictive modelling in ALS by reducing the variability of estimated parameters at the cost of a slight increase in bias. This onset-anchored model is extremely useful if predictions are desired directly after a single baseline measure (such as at the first day of a clinical trial), a feat that would be very difficult without the onset-anchor. This approach could be useful in modelling other diseases that have bounded progression scales (e.g. Parkinson's disease, Huntington's disease, or inclusion-body myositis). It is our hope that this model can be used by clinicians and statisticians to improve the efficacy of clinical trials and aid in finding treatments for ALS.
肌萎缩侧索硬化症(ALS),又称葛雷克氏症,是一种罕见疾病,具有极强的个体间变异性,尤其是在疾病进展速度方面。这使得对患者的疾病进展建模变得非常困难,而疾病进展是通过肌萎缩侧索硬化功能评定量表(ALSFRS)来衡量的。
我们从汇集资源开放获取肌萎缩侧索硬化临床试验数据库(一个由各种肌萎缩侧索硬化临床试验数据组成的数据库)中获取了 ALS 患者的数据。由于 ALSFRS 的典型线性性,我们考虑了几种贝叶斯层次线性模型。这些模型包括一个混合模型(用于解释“快速”和“缓慢”ALS 进展者的两种潜在类别)以及一个起始锚定模型,其中利用疾病起始时间添加了一个额外的人工数据点,以提高预测性能。
与贝叶斯层次线性模型或混合模型相比,起始锚定模型的后验预测均方误差分布有明显的减少。除了疾病起始时间之外,没有其他协变量可以在贝叶斯层次线性模型或起始锚定模型中持续提高预测性能。
在患者数据中添加一个额外的人工数据点(起始锚点)可以极大地改善 ALS 的预测建模,方法是降低估计参数的变异性,代价是略微增加偏差。如果需要直接在单个基线测量后(例如在临床试验的第一天)进行预测,那么这个起始锚定模型非常有用,而没有起始锚点的话,这将是非常困难的。这种方法在建模其他进展尺度有界的疾病(例如帕金森病、亨廷顿病或包涵体肌炎)时可能很有用。我们希望该模型能够被临床医生和统计学家用于提高临床试验的疗效,并帮助寻找 ALS 的治疗方法。