Neslusan Cheryl, Teschemaker Anna, Willis Michael, Johansen Pierre, Vo Lien
Janssen Global Services, LLC, Raritan, NJ, USA.
The Swedish Institute for Health Economics, Lund, Sweden.
Diabetes Ther. 2018 Apr;9(2):565-581. doi: 10.1007/s13300-018-0371-y. Epub 2018 Feb 6.
Agents that inhibit sodium glucose co-transporter 2 (SGLT2), including canagliflozin and dapagliflozin, are approved in the United States for the treatment of adults with type 2 diabetes mellitus (T2DM). SGLT2 inhibition lowers blood glucose by increasing urinary glucose excretion, which leads to a mild osmotic diuresis and a net loss of calories that are associated with reductions in body weight and blood pressure. This analysis evaluated the cost-effectiveness of canagliflozin 300 mg versus dapagliflozin 10 mg in patients with T2DM inadequately controlled with metformin in the United States.
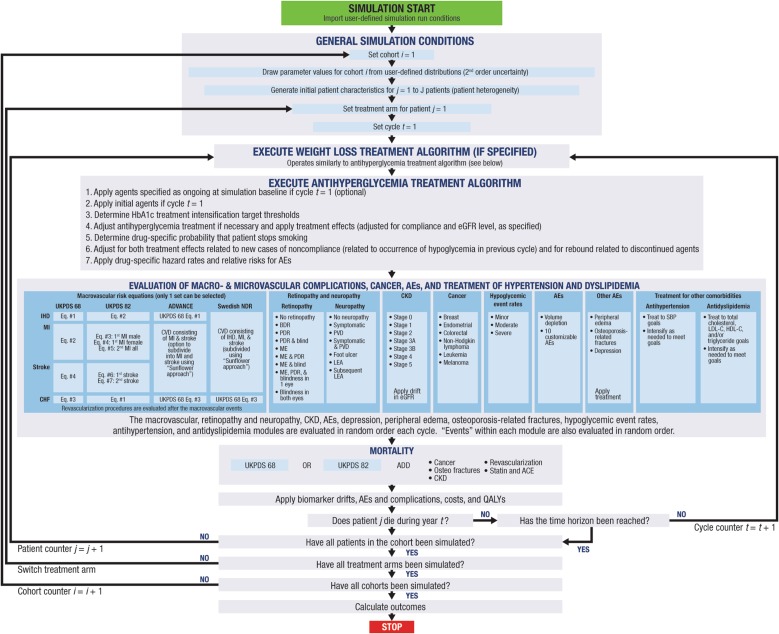
A 30-year cost-effectiveness analysis was performed using the validated Economic and Health Outcomes Model of T2DM (ECHO-T2DM) from the perspective of the third-party health care system in the United States. Patient demographics, biomarker values, and treatment effects for the ECHO-T2DM model were sourced primarily from a network meta-analysis (NMA) that included studies of canagliflozin and dapagliflozin in patients with T2DM on background metformin. Costs were derived from sources specific to the United States. Outcomes and costs were discounted at 3%. Sensitivity analyses that varied key model parameters were conducted.
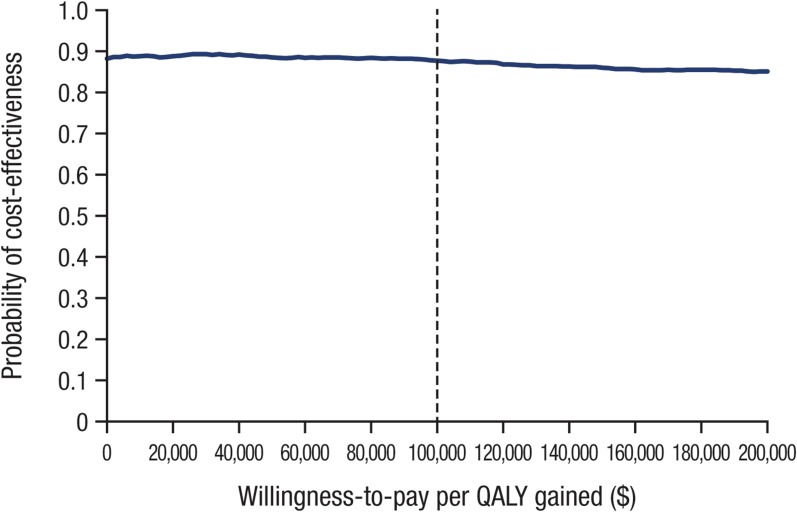
Canagliflozin 300 mg dominated dapagliflozin 10 mg as an add-on to metformin over 30 years, with an estimated cost offset of $13,991 and a quality-adjusted life-year gain of 0.08 versus dapagliflozin 10 mg. Results were driven by the better HbA1c lowering achieved with canagliflozin, which translated to less need for insulin rescue therapy. Findings from sensitivity analyses were consistent with the base case.
These results suggest that canagliflozin 300 mg is likely to provide better health outcomes at a lower overall cost than dapagliflozin 10 mg in patients with T2DM inadequately controlled with metformin from the perspective of the United States health care system.
Janssen Scientific Affairs, LLC and Janssen Global Services, LLC.
抑制钠葡萄糖协同转运蛋白2(SGLT2)的药物,包括卡格列净和达格列净,在美国已被批准用于治疗成年2型糖尿病(T2DM)患者。SGLT2抑制通过增加尿糖排泄来降低血糖,这会导致轻度渗透性利尿以及与体重和血压降低相关的热量净损失。本分析评估了在美国二甲双胍治疗控制不佳的T2DM患者中,300毫克卡格列净与10毫克达格列净的成本效益。
从美国第三方医疗保健系统的角度,使用经过验证的T2DM经济和健康结果模型(ECHO-T2DM)进行了为期30年的成本效益分析。ECHO-T2DM模型的患者人口统计学、生物标志物值和治疗效果主要来自一项网络荟萃分析(NMA),该分析纳入了在接受二甲双胍治疗的T2DM患者中使用卡格列净和达格列净的研究。成本来自美国特有的来源。结果和成本按3%进行贴现。进行了改变关键模型参数的敏感性分析。
在30年的时间里,作为二甲双胍的附加治疗药物,300毫克卡格列净优于10毫克达格列净,估计成本抵消为13,991美元,与10毫克达格列净相比,质量调整生命年增加0.08。结果是由卡格列净在降低糖化血红蛋白(HbA1c)方面表现更好所驱动的,这意味着对胰岛素挽救治疗的需求减少。敏感性分析的结果与基础病例一致。
这些结果表明,从美国医疗保健系统的角度来看,在二甲双胍治疗控制不佳的T2DM患者中,300毫克卡格列净可能以低于10毫克达格列净的总体成本提供更好的健康结果。
杨森科学事务有限责任公司和杨森全球服务有限责任公司。