Kosiborod Mikhail, Cavender Matthew A, Fu Alex Z, Wilding John P, Khunti Kamlesh, Holl Reinhard W, Norhammar Anna, Birkeland Kåre I, Jørgensen Marit Eika, Thuresson Marcus, Arya Niki, Bodegård Johan, Hammar Niklas, Fenici Peter
From Saint Luke's Mid America Heart Institute and University of Missouri-Kansas City (M.K.); University of North Carolina, Chapel Hill (M.A.C.); Georgetown University Medical Center, Washington, DC (A.Z.F.); University of Liverpool, United Kingdom (J.P.W.); University of Leicester, United Kingdom (K.K.); University of Ulm, Germany (R.W.H.); Karolinska Institutet, Stockholm, Sweden (A.N., N.H.); University of Oslo, Norway (K.I.B.); Oslo University Hospital, Norway (K.I.B.); Steno Diabetes Center, Copenhagen, Gentofte, Denmark (M.E.J.); National Institute of Public Health, Southern Denmark University, Copenhagen (M.E.J.); Statisticon AB, Uppsala, Sweden (M.T.); AstraZeneca, Gaithersburg, MD (N.A.); AstraZeneca, Oslo, Norway (J.B.); AstraZeneca Gothenburg, Sweden (N.H.); and AstraZeneca, Cambridge, United Kingdom (P.F.).
Circulation. 2017 Jul 18;136(3):249-259. doi: 10.1161/CIRCULATIONAHA.117.029190. Epub 2017 May 18.
Reduction in cardiovascular death and hospitalization for heart failure (HHF) was recently reported with the sodium-glucose cotransporter-2 inhibitor (SGLT-2i) empagliflozin in patients with type 2 diabetes mellitus who have atherosclerotic cardiovascular disease. We compared HHF and death in patients newly initiated on any SGLT-2i versus other glucose-lowering drugs in 6 countries to determine if these benefits are seen in real-world practice and across SGLT-2i class.
Data were collected via medical claims, primary care/hospital records, and national registries from the United States, Norway, Denmark, Sweden, Germany, and the United Kingdom. Propensity score for SGLT-2i initiation was used to match treatment groups. Hazard ratios for HHF, death, and their combination were estimated by country and pooled to determine weighted effect size. Death data were not available for Germany.
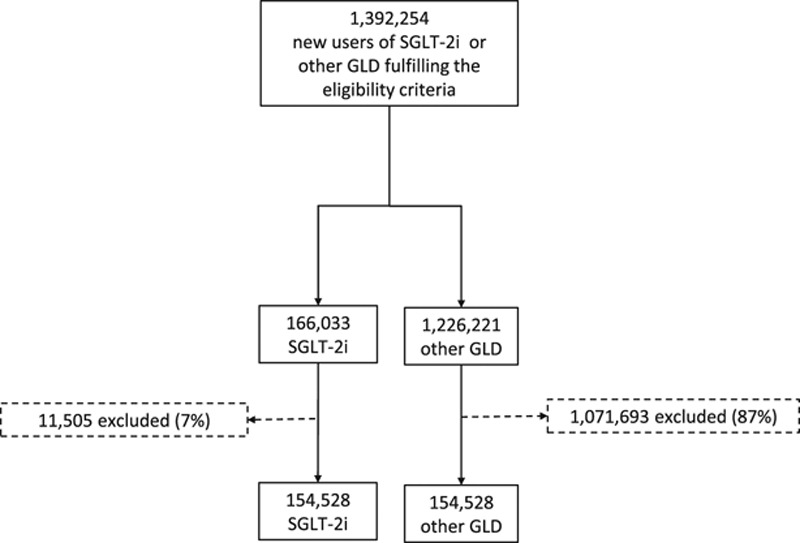
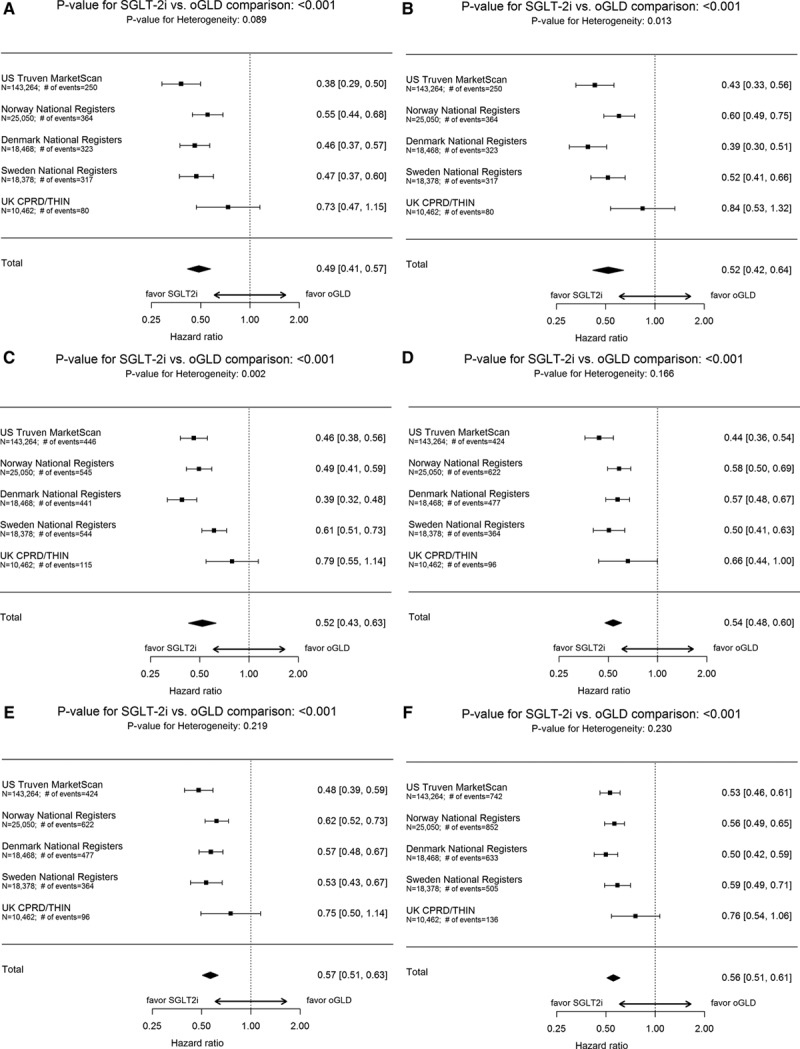
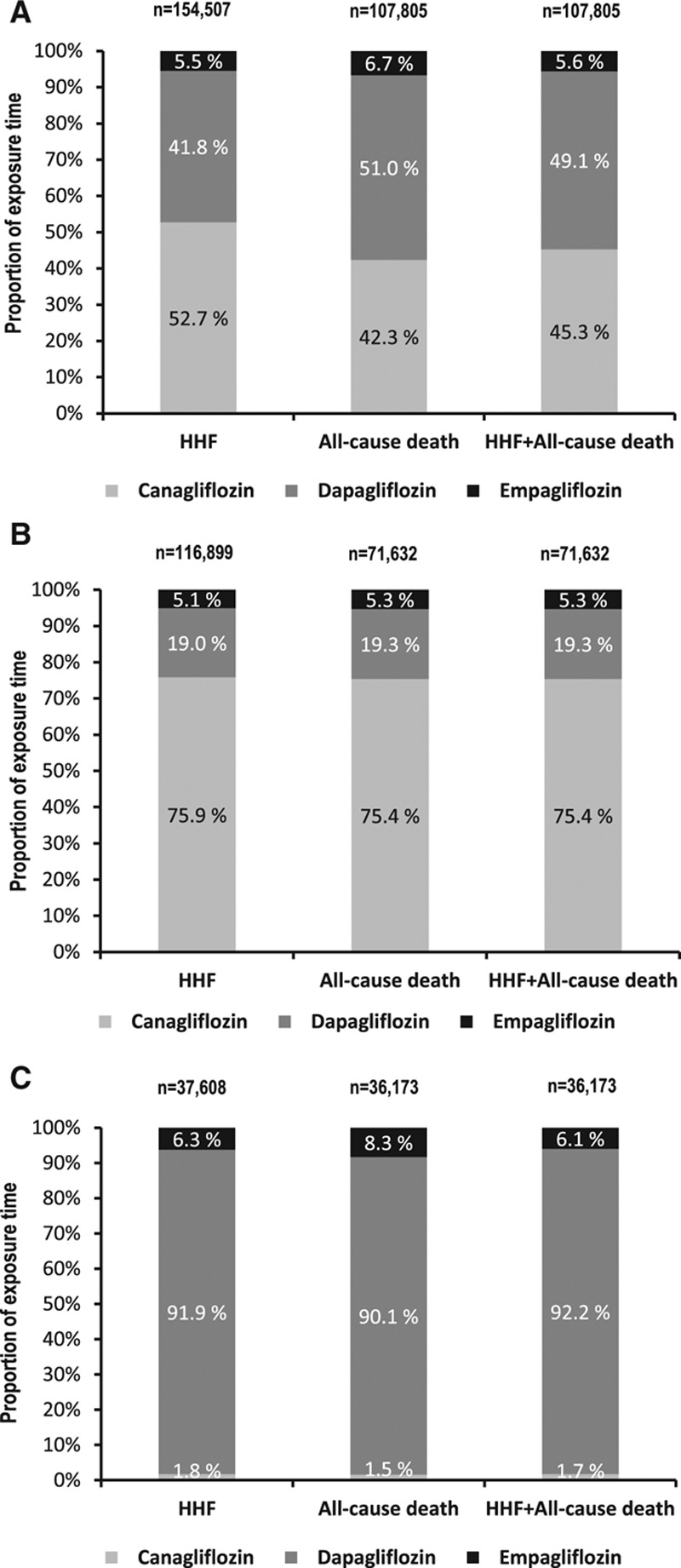
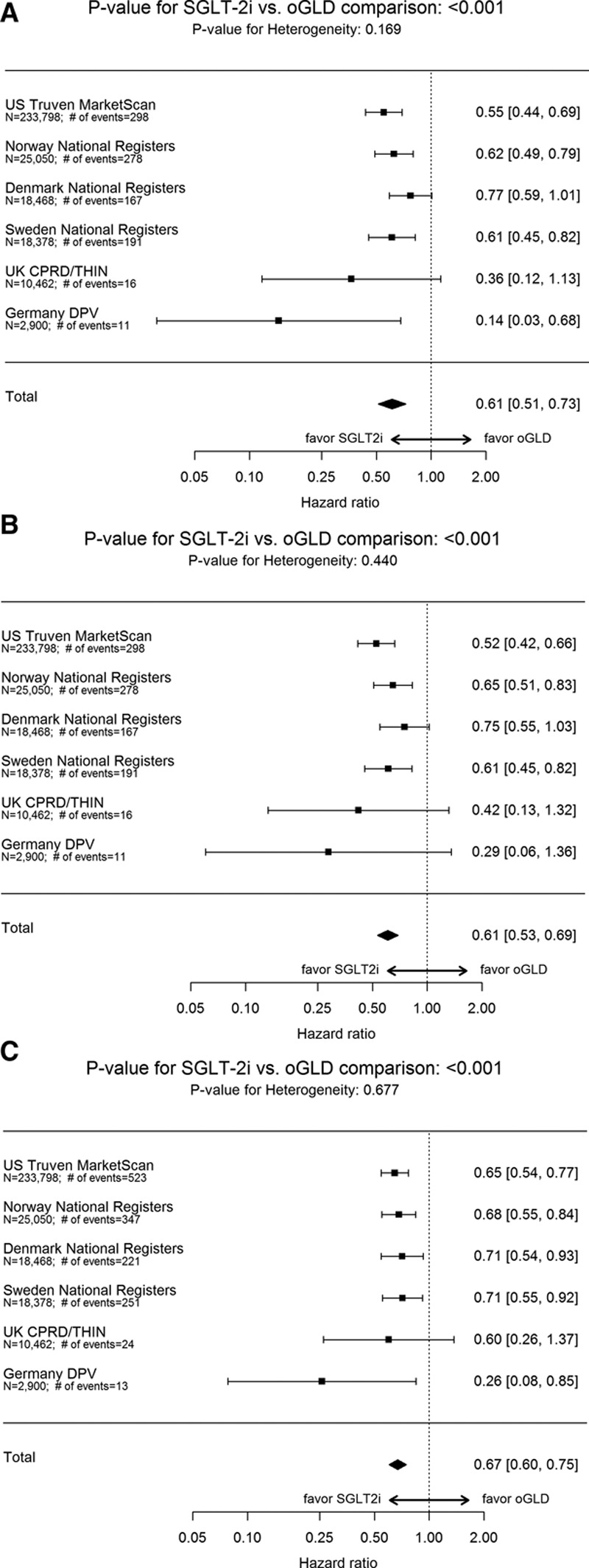
After propensity matching, there were 309 056 patients newly initiated on either SGLT-2i or other glucose-lowering drugs (154 528 patients in each treatment group). Canagliflozin, dapagliflozin, and empagliflozin accounted for 53%, 42%, and 5% of the total exposure time in the SGLT-2i class, respectively. Baseline characteristics were balanced between the 2 groups. There were 961 HHF cases during 190 164 person-years follow-up (incidence rate, 0.51/100 person-years). Of 215 622 patients in the United States, Norway, Denmark, Sweden, and the United Kingdom, death occurred in 1334 (incidence rate, 0.87/100 person-years), and HHF or death in 1983 (incidence rate, 1.38/100 person-years). Use of SGLT-2i, versus other glucose-lowering drugs, was associated with lower rates of HHF (hazard ratio, 0.61; 95% confidence interval, 0.51-0.73; <0.001); death (hazard ratio, 0.49; 95% confidence interval, 0.41-0.57; <0.001); and HHF or death (hazard ratio, 0.54; 95% confidence interval, 0.48-0.60; <0.001) with no significant heterogeneity by country.
In this large multinational study, treatment with SGLT-2i versus other glucose-lowering drugs was associated with a lower risk of HHF and death, suggesting that the benefits seen with empagliflozin in a randomized trial may be a class effect applicable to a broad population of patients with type 2 diabetes mellitus in real-world practice.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT02993614.
近期有报道称,对于患有动脉粥样硬化性心血管疾病的2型糖尿病患者,钠-葡萄糖协同转运蛋白2抑制剂(SGLT-2i)恩格列净可降低心血管死亡风险以及因心力衰竭(HHF)住院的风险。我们比较了6个国家中开始使用任何一种SGLT-2i的患者与开始使用其他降糖药物的患者发生HHF和死亡的情况,以确定在实际临床实践中以及在整个SGLT-2i类别中是否都能观察到这些益处。
通过医疗理赔、初级保健/医院记录以及来自美国、挪威、丹麦、瑞典、德国和英国的国家登记处收集数据。使用SGLT-2i起始治疗的倾向评分来匹配治疗组。按国家估算HHF、死亡及其合并事件的风险比,并汇总以确定加权效应大小。德国没有死亡数据。
倾向匹配后,共有309056例患者开始使用SGLT-2i或其他降糖药物(每个治疗组各154528例患者)。在SGLT-2i类别中,卡格列净、达格列净和恩格列净分别占总暴露时间的53%、42%和5%。两组之间的基线特征均衡。在190164人年的随访期间,共发生961例HHF病例(发病率为0.51/100人年)。在美国、挪威、丹麦、瑞典和英国的215622例患者中,有1334例死亡(发病率为0.87/100人年),1983例发生HHF或死亡(发病率为1.38/100人年)。与其他降糖药物相比,使用SGLT-2i可降低HHF发生率(风险比为0.61;95%置信区间为0.51-0.73;P<0.001)、死亡发生率(风险比为0.49;95%置信区间为0.41-0.57;P<0.001)以及HHF或死亡的发生率(风险比为0.54;95%置信区间为0.48-0.60;P<0.001),且各国之间无显著异质性。
在这项大型跨国研究中,与其他降糖药物相比,使用SGLT-2i治疗可降低HHF和死亡风险,这表明恩格列净在随机试验中显示的益处可能是一种类别效应,适用于实际临床实践中广泛的2型糖尿病患者群体。