Stack Austin G, Alghali Ahmed, Li Xia, Ferguson John P, Casserly Liam F, Cronin Cornelius J, Reddan Donal N, Hussein Wael, Elsayed Mohamed E
Department of Nephrology, University Hospital Limerick, Limerick, Ireland.
Graduate Entry Medical School, University of Limerick, Limerick, Ireland.
Clin Kidney J. 2018 Feb;11(1):99-107. doi: 10.1093/ckj/sfx060. Epub 2017 Jul 13.
Although anaemia is a common complication of advanced chronic kidney disease (CKD), knowledge of quality of care and management practices in specialist clinics varies. We examined anaemia practices at specialist nephrology clinics within the Irish health system and evaluated the opinions of practicing nephrologists.
A multicentre cross-sectional study was conducted at specialist nephrology clinics across six geographic regions in Ireland. Clinical characteristics and treatment practices were evaluated in a sample of 530 patients with CKD. An accompanying national survey questionnaire captured opinions and treatment strategies of nephrologists on anaemia management.
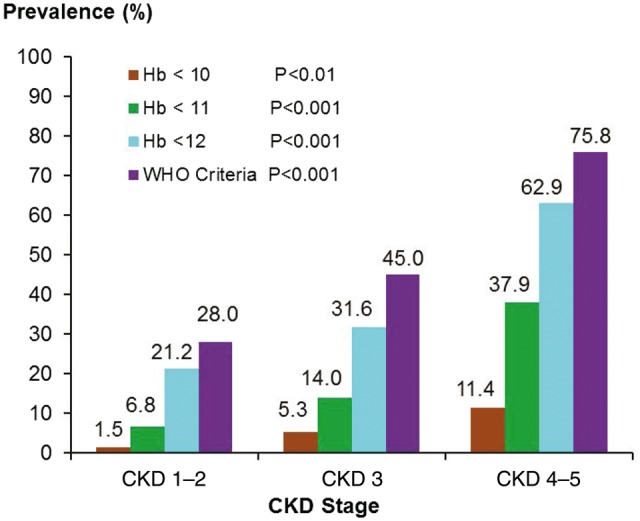
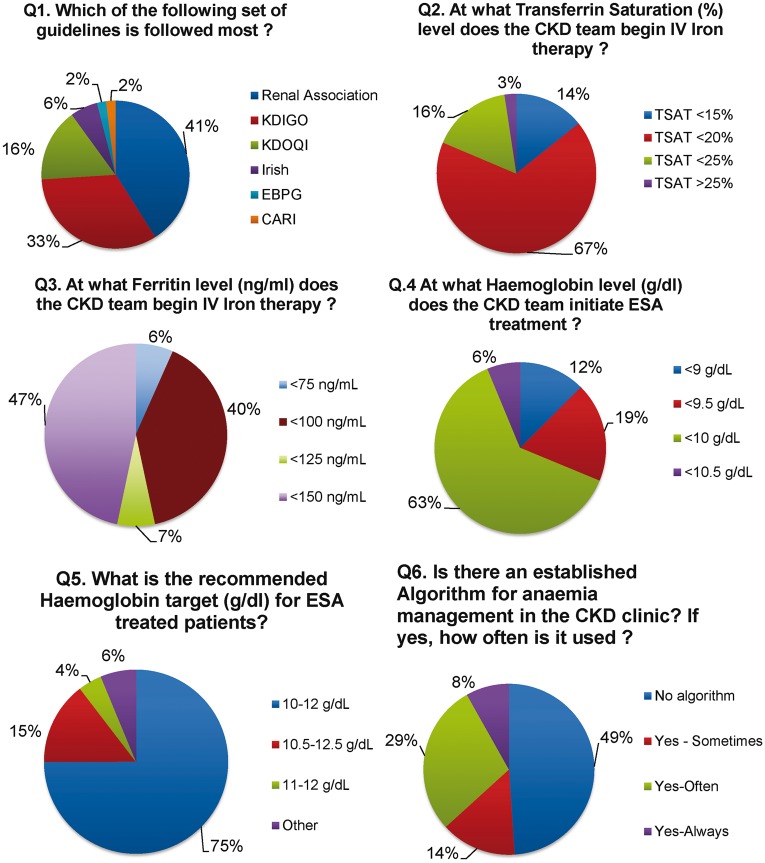
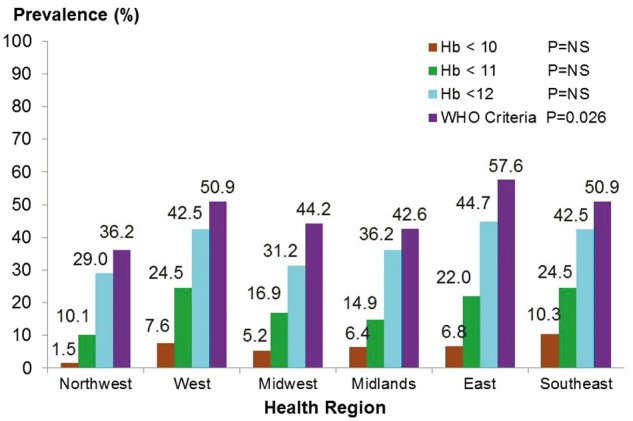
The prevalence of anaemia [defined as haemoglobin (Hb) <12.0 g/dL] was 37.8%, which increased significantly with advancing CKD (from 21% to 63%; P < 0.01) and varied across clinical sites (from 36% to 62%; P < 0.026). Iron deficiency (ID) was present in 46% of all patients tested and 86% of them were not on treatment. More than 45% of anaemic patients were not tested for ID. Respondents differed in their selection of clinical guidelines, threshold targets for erythropoiesis-stimulating agent (ESA) and intravenous iron therapy and anaemia management algorithms were absent in 47% of the clinics. The unexpectedly low rates of ESA use (4.7%) and iron therapy (10.2%) in clinical practice were in contrast to survey responses where 63% of nephrologists indicated ESA therapy initiation when Hb was <10.0 g/dL and 46% indicated commencement of iron therapy for ferritin <150 ng/mL.
This study highlights substantial variability in the management of anaemia and ID at specialist nephrology clinics with low testing rates for ID, high rates of anaemia and ID and underutilization of effective treatments. Variability in the adoption and implementation of different clinical guidelines was evident.
尽管贫血是晚期慢性肾脏病(CKD)的常见并发症,但专科诊所的护理质量和管理实践的认知存在差异。我们研究了爱尔兰卫生系统内专科肾脏病诊所的贫血诊疗实践,并评估了执业肾脏病医生的意见。
在爱尔兰六个地理区域的专科肾脏病诊所进行了一项多中心横断面研究。对530例CKD患者的样本进行了临床特征和治疗实践评估。同时进行的一项全国调查问卷收集了肾脏病医生对贫血管理的意见和治疗策略。
贫血(定义为血红蛋白(Hb)<12.0 g/dL)的患病率为37.8%,随着CKD进展显著增加(从21%增至63%;P<0.01),且在各临床机构有所不同(从36%至62%;P<0.026)。46%接受检测的患者存在缺铁(ID),其中86%未接受治疗。超过45%的贫血患者未接受ID检测。受访者在临床指南的选择、促红细胞生成素(ESA)和静脉铁剂治疗的阈值目标方面存在差异,47%的诊所没有贫血管理算法。临床实践中ESA使用(4.7%)和铁剂治疗(10.2%)的意外低发生率与调查结果形成对比,调查中63%的肾脏病医生表示当Hb<10.0 g/dL时开始ESA治疗,46%表示当铁蛋白<150 ng/mL时开始铁剂治疗。
本研究突出了专科肾脏病诊所在贫血和ID管理方面存在的显著差异,ID检测率低、贫血和ID发生率高以及有效治疗利用不足。不同临床指南的采用和实施存在差异。