Amstutz Alain, Nsakala Bienvenu Lengo, Vanobberghen Fiona, Muhairwe Josephine, Glass Tracy Renée, Achieng Beatrice, Sepeka Mamorena, Tlali Katleho, Sao Lebohang, Thin Kyaw, Klimkait Thomas, Battegay Manuel, Labhardt Niklaus Daniel
Clinical Research Unit, Department of Medicine, Swiss Tropical and Public Health Institute, Socinstrasse 57, 4051, Basel, Switzerland.
University of Basel, 4051, Basel, Switzerland.
BMC Infect Dis. 2018 Feb 12;18(1):76. doi: 10.1186/s12879-018-2979-y.
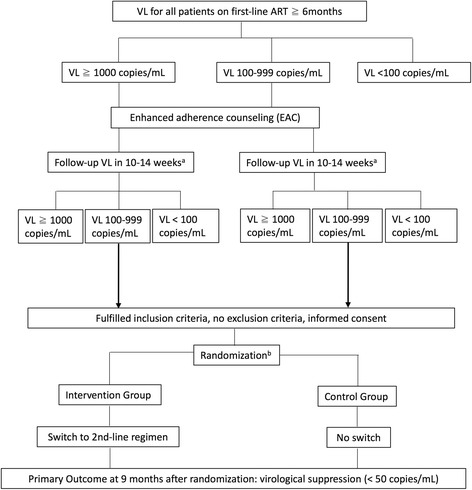
The World Health Organization (WHO) recommends viral load (VL) measurement as the preferred monitoring strategy for HIV-infected individuals on antiretroviral therapy (ART) in resource-limited settings. The new WHO guidelines 2016 continue to define virologic failure as two consecutive VL ≥1000 copies/mL (at least 3 months apart) despite good adherence, triggering switch to second-line therapy. However, the threshold of 1000 copies/mL for defining virologic failure is based on low-quality evidence. Observational studies have shown that individuals with low-level viremia (measurable but below 1000 copies/mL) are at increased risk for accumulation of resistance mutations and subsequent virologic failure. The SESOTHO trial assesses a lower threshold for switch to second-line ART in patients with sustained unsuppressed VL.
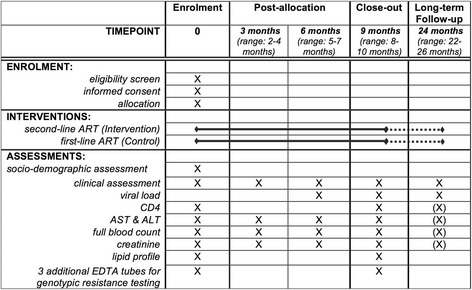
In this multicenter, parallel-group, open-label, randomized controlled trial conducted in Lesotho, patients on first-line ART with two consecutive unsuppressed VL measurements ≥100 copies/mL, where the second VL is between 100 and 999 copies/mL, will either be switched to second-line ART immediately (intervention group) or not be switched (standard of care, according to WHO guidelines). The primary endpoint is viral resuppression (VL < 50 copies/mL) 9 months after randomization. We will enrol 80 patients, giving us 90% power to detect a difference of 35% in viral resuppression between the groups (assuming two-sided 5% alpha error). For our primary analysis, we will use a modified intention-to-treat set, with those lost to care, death, or crossed over considered failure to resuppress, and using logistic regression models adjusted for the prespecified stratification variables.
The SESOTHO trial challenges the current WHO guidelines, assessing an alternative, lower VL threshold for patients with unsuppressed VL on first-line ART. This trial will provide data to inform future WHO guidelines on VL thresholds to recommend switch to second-line ART.
ClinicalTrials.gov ( NCT03088241 ), registered May 05, 2017.
世界卫生组织(WHO)建议,在资源有限的环境中,对于接受抗逆转录病毒治疗(ART)的HIV感染者,病毒载量(VL)检测是首选的监测策略。2016年WHO新指南继续将病毒学失败定义为,尽管依从性良好,但连续两次VL≥1000拷贝/毫升(至少间隔3个月),此时需转而接受二线治疗。然而,将病毒学失败的阈值设定为1000拷贝/毫升是基于低质量证据。观察性研究表明,病毒血症水平较低(可检测到但低于1000拷贝/毫升)的个体出现耐药突变积累及随后病毒学失败的风险增加。SESOTHO试验评估了持续未抑制VL的患者转而接受二线ART的较低阈值。
在莱索托进行的这项多中心、平行组、开放标签随机对照试验中,一线ART患者连续两次未抑制的VL测量值≥100拷贝/毫升,且第二次VL在100至999拷贝/毫升之间,这些患者将立即转而接受二线ART(干预组),或不进行转换(根据WHO指南作为标准治疗)。主要终点是随机分组9个月后病毒重新抑制(VL<50拷贝/毫升)。我们将招募80名患者,有90%的把握检测出两组之间病毒重新抑制率相差35%(假设双侧α错误为5%)。对于我们的主要分析,我们将使用一个修改后的意向性分析集,将失访、死亡或交叉的患者视为未能重新抑制,并使用针对预先指定的分层变量进行调整的逻辑回归模型。
SESOTHO试验对当前WHO指南提出了挑战,评估了一线ART中VL未抑制患者的另一个更低的VL阈值。该试验将提供数据,为WHO未来关于推荐转而接受二线ART的VL阈值指南提供参考。
ClinicalTrials.gov(NCT03088241),于2017年5月5日注册。