Université Clermont Auvergne, CHU Clermont-Ferrand, Service de radiologie, Clermont-Ferrand 63000, France.
CHU de Reims, Service d'Hépato-Gastro Entérologie, Reims 51100, France.
World J Gastroenterol. 2018 Feb 7;24(5):641-650. doi: 10.3748/wjg.v24.i5.641.
To assess magnetic resonance imaging (MRI) and faecal calprotectin to detect endoscopic postoperative recurrence in patients with Crohn's disease (CD).
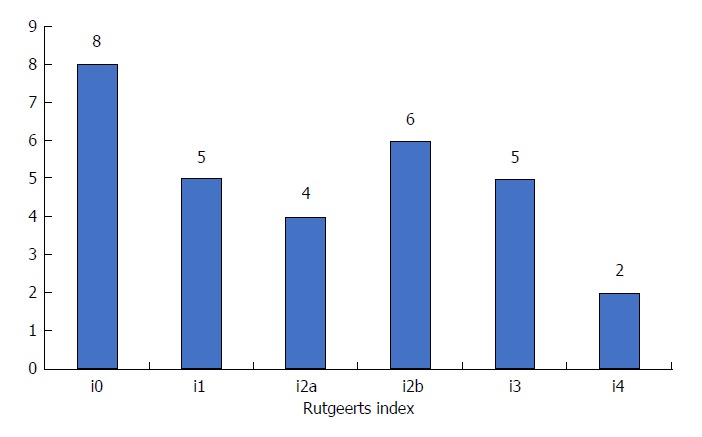
From two tertiary centers, all patients with CD who underwent ileocolonic resection were consecutively and prospectively included. All the patients underwent MRI and endoscopy within the first year after surgery or after the restoration of intestinal continuity [median = 6 mo (5.0-9.3)]. The stools were collected the day before the colonoscopy to evaluate faecal calprotectin level. Endoscopic postoperative recurrence (POR) was defined as Rutgeerts' index ≥ i2b. The MRI was analyzed independently by two radiologists blinded from clinical data.
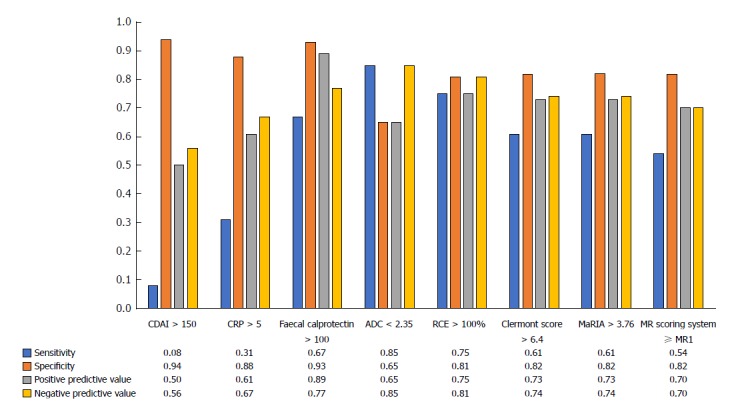
Apparent diffusion coefficient (ADC) was lower in patients with endoscopic POR compared to those with no recurrence (2.03 ± 0.32 2.27 ± 0.38 × 10 mm²/s, = 0.032). Clermont score (10.4 ± 5.8 7.4 ± 4.5, = 0.038) and relative contrast enhancement (RCE) (129.4% ± 62.8% 76.4% ± 32.6%, = 0.007) were significantly associated with endoscopic POR contrary to the magnetic resonance index of activity (MaRIA) (7.3 ± 4.5 4.8 ± 3.7; = 0.15) and MR scoring system ( = 0.056). ADC < 2.35 × 10 mm²/s [sensitivity = 0.85, specificity = 0.65, positive predictive value (PPV) = 0.85, negative predictive value (NPV) = 0.65] and RCE > 100% (sensitivity = 0.75, specificity = 0.81, PPV = 0.75, NPV = 0.81) were the best cut-off values to identify endoscopic POR. Clermont score > 6.4 (sensitivity = 0.61, specificity = 0.82, PPV = 0.73, NPV = 0.74), MaRIA > 3.76 (sensitivity = 0.61, specificity = 0.82, PPV = 0.73, NPV = 0.74) and a MR scoring system ≥ MR1 (sensitivity = 0.54, specificity = 0.82, PPV = 0.70, and NPV = 0.70) demonstrated interesting performances to detect endoscopic POR. Faecal calprotectin values were significantly higher in patients with endoscopic POR (114 ± 54.5 μg/g 354.8 ± 432.5 μg/g; = 0.0075). Faecal calprotectin > 100 μg/g demonstrated high performances to detect endoscopic POR (sensitivity = 0.67, specificity = 0.93, PPV = 0.89 and NPV = 0.77).
Faecal calprotectin and MRI are two reliable tools to detect endoscopic POR in patients with CD.
评估磁共振成像(MRI)和粪便钙卫蛋白在克罗恩病(CD)患者内镜术后复发中的作用。
从两个三级中心连续前瞻性纳入所有接受回肠结肠切除术的 CD 患者。所有患者在术后 1 年内或肠道连续性恢复后(中位数=6 个月(5.0-9.3))进行 MRI 和内镜检查。结肠镜检查前一天收集粪便,以评估粪便钙卫蛋白水平。内镜术后复发(POR)定义为 Rutgeerts 指数≥i2b。MRI 由两名独立于临床数据的放射科医生进行分析。
与无复发患者相比,内镜 POR 患者的表观扩散系数(ADC)较低(2.03±0.32 vs. 2.27±0.38×10mm²/s,=0.032)。Clermont 评分(10.4±5.8 vs. 7.4±4.5,=0.038)和相对对比增强(RCE)(129.4%±62.8% vs. 76.4%±32.6%,=0.007)与内镜 POR 显著相关,而活动磁共振指数(MaRIA)(7.3±4.5 vs. 4.8±3.7,=0.15)和磁共振评分系统(=0.056)则无显著相关性。ADC<2.35×10mm²/s[灵敏度=0.85,特异性=0.65,阳性预测值(PPV)=0.85,阴性预测值(NPV)=0.65]和 RCE>100%(灵敏度=0.75,特异性=0.81,PPV=0.75,NPV=0.81)是识别内镜 POR 的最佳截断值。Clermont 评分>6.4(灵敏度=0.61,特异性=0.82,PPV=0.73,NPV=0.74)、MaRIA>3.76(灵敏度=0.61,特异性=0.82,PPV=0.73,NPV=0.74)和磁共振评分系统≥MR1(灵敏度=0.54,特异性=0.82,PPV=0.70,NPV=0.70)在检测内镜 POR 方面表现出有趣的性能。内镜 POR 患者粪便钙卫蛋白值显著升高(114±54.5μg/g vs. 354.8±432.5μg/g;=0.0075)。粪便钙卫蛋白>100μg/g 对检测内镜 POR 具有较高的性能(灵敏度=0.67,特异性=0.93,PPV=0.89,NPV=0.77)。
粪便钙卫蛋白和 MRI 是检测 CD 患者内镜 POR 的两种可靠工具。