From the Department of Pharmacology (B.H., J.B., K.S.G., L.T.I., Y.C.-I., D.M.B.), School of Medicine, Dean's Office (L.T.), Surgical Research Facility, School of Medicine (W.T.F.), Department of Biomedical Engineering (Y.C.-I.), Department of Internal Medicine/Cardiology (Y.C.-I.), University of California, Davis; Echocardiography Laboratory, University of California, Davis Medical Center, Sacramento (L.M.M.); and Department of Medicine, University of Alabama at Birmingham (S.M.P.).
Circ Arrhythm Electrophysiol. 2018 Feb;11(2):e005852. doi: 10.1161/CIRCEP.117.005852.
Electrophysiological remodeling and increased susceptibility for cardiac arrhythmias are hallmarks of heart failure (HF). Ventricular action potential duration (APD) is typically prolonged in HF, with reduced repolarization reserve. However, underlying K current changes are often measured in nonphysiological conditions (voltage clamp, low pacing rates, cytosolic Ca buffers).
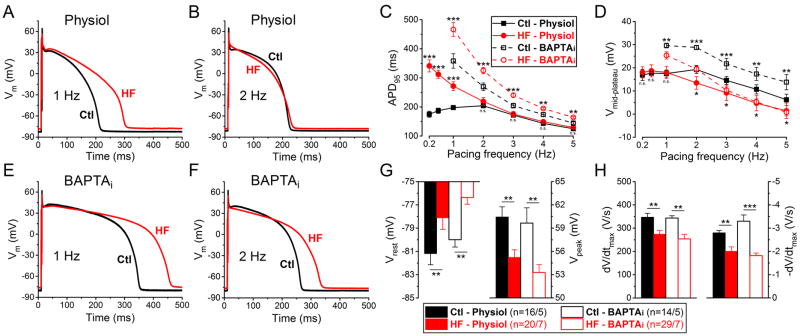
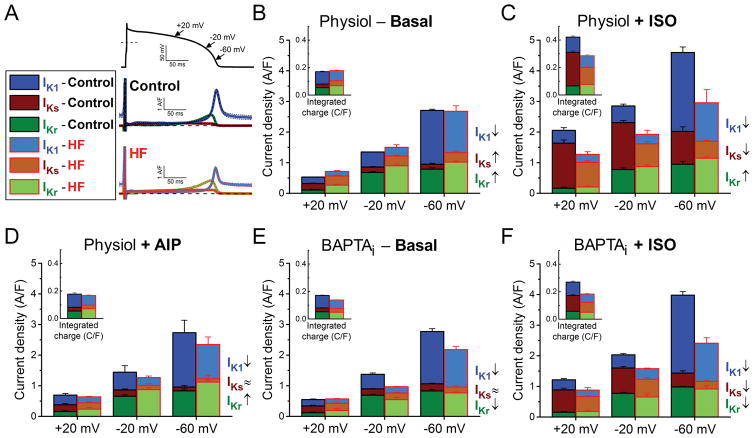
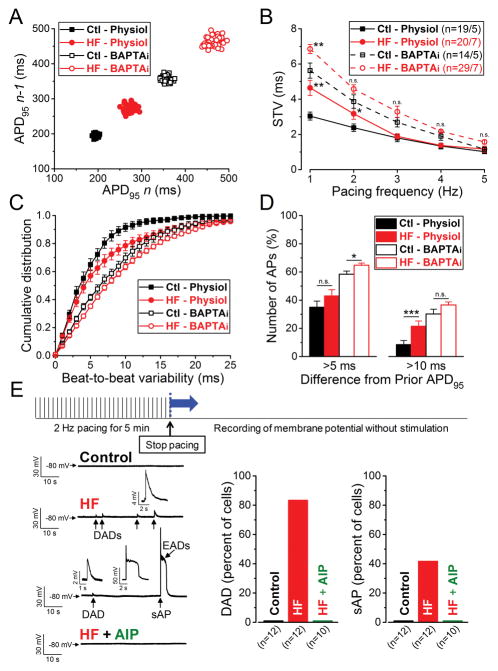
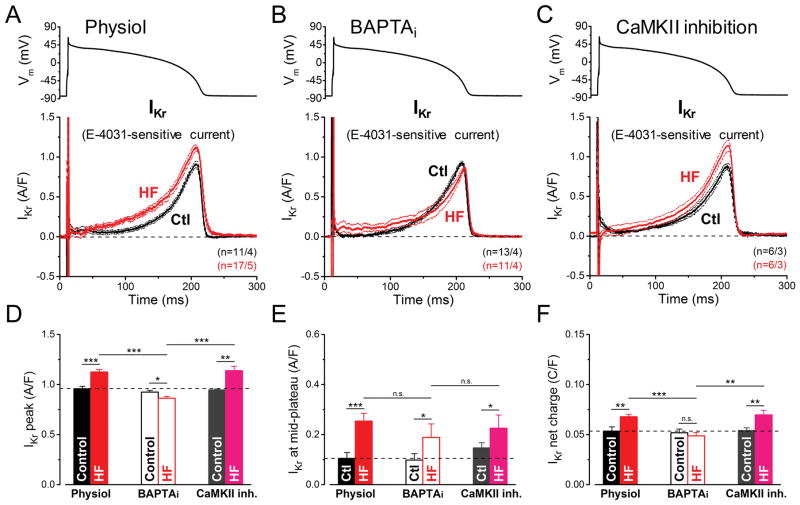
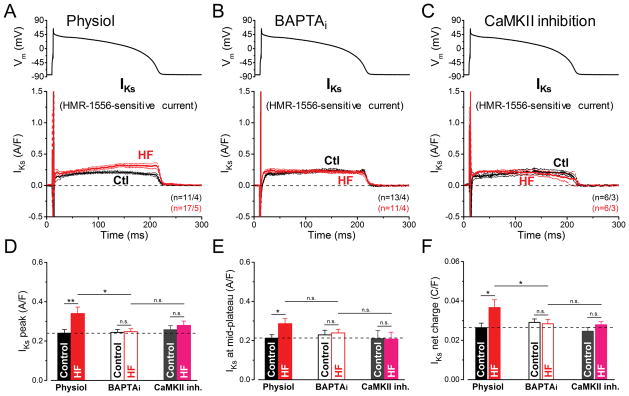
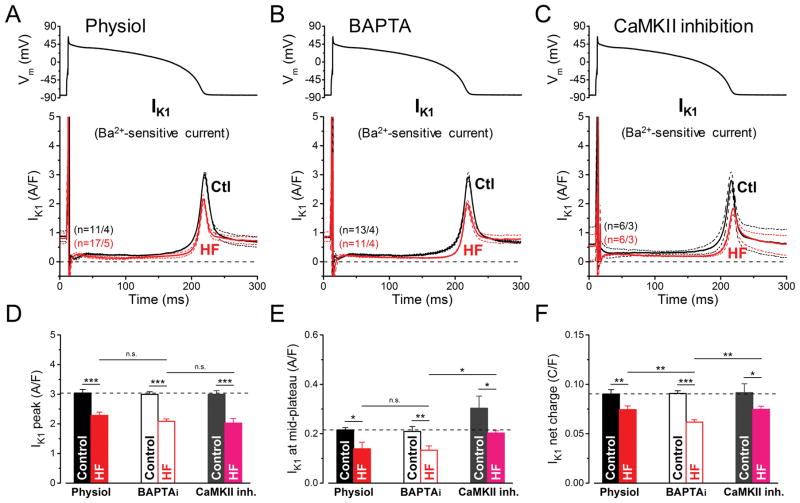
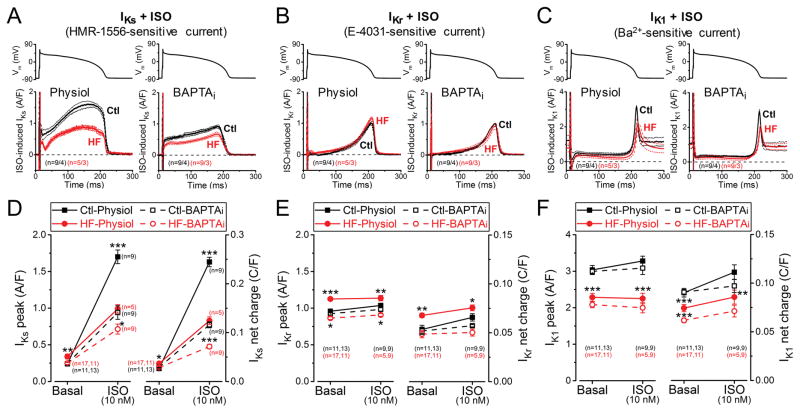
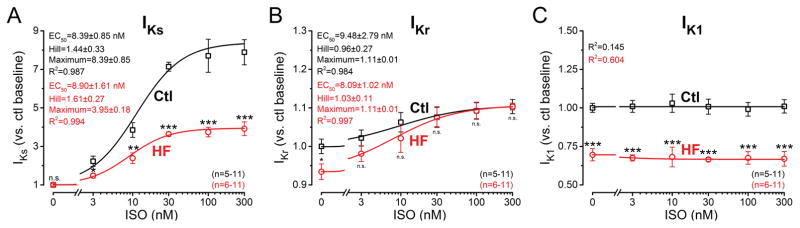
We measured the major K currents (, , and ) and their Ca- and β-adrenergic dependence in rabbit ventricular myocytes in chronic pressure/volume overload-induced HF (versus age-matched controls). APD was significantly prolonged only at lower pacing rates (0.2-1 Hz) in HF under physiological ionic conditions and temperature. However, when cytosolic Ca was buffered, APD prolongation in HF was also significant at higher pacing rates. Beat-to-beat variability of APD was also significantly increased in HF. Both and were significantly upregulated in HF under action potential clamp, but only when cytosolic Ca was not buffered. CaMKII (Ca/calmodulin-dependent protein kinase II) inhibition abolished upregulation in HF, but it did not affect . response to β-adrenergic stimulation was also significantly diminished in HF. was also decreased in HF regardless of Ca buffering, CaMKII inhibition, or β-adrenergic stimulation.
At baseline Ca-dependent upregulation of and in HF counterbalances the reduced , maintaining repolarization reserve (especially at higher heart rates) in physiological conditions, unlike conditions of strong cytosolic Ca buffering. However, under β-adrenergic stimulation, reduced responsiveness severely limits integrated repolarizing K current and repolarization reserve in HF. This would increase arrhythmia propensity in HF, especially during adrenergic stress.
电生理重构和心脏性心律失常易感性增加是心力衰竭(HF)的特征。HF 时心室动作电位时程(APD)通常延长,复极储备减少。然而,潜在的 K 电流变化通常在非生理条件下(电压钳、低起搏率、细胞溶质 Ca 缓冲液)进行测量。
我们在慢性压力/容量超负荷诱导的 HF 兔心室肌细胞(与年龄匹配的对照组相比)中测量了主要 K 电流(,,和)及其 Ca 和 β-肾上腺素依赖性。在生理离子条件和温度下,仅在较低的起搏率(0.2-1 Hz)下,HF 时 APD 才显著延长。然而,当细胞溶质 Ca 被缓冲时,HF 中的 APD 延长在较高的起搏率下也很明显。APD 的搏动间变异性在 HF 中也显著增加。在动作电位钳制下,HF 中的 和 均显著上调,但仅在未缓冲细胞溶质 Ca 时。CaMKII(Ca/钙调蛋白依赖性蛋白激酶 II)抑制消除了 HF 中 上调,但不影响 。HF 中 β-肾上腺素刺激的 反应也明显减弱。无论 Ca 缓冲、CaMKII 抑制还是 β-肾上腺素刺激,HF 中 也减少。
在基线 Ca 依赖性上调的情况下,HF 中 和 的上调可代偿减少的 ,从而在生理条件下保持复极储备(尤其是在较高的心率下),与强细胞溶质 Ca 缓冲条件不同。然而,在 β-肾上腺素刺激下,减少的 反应性严重限制了 HF 中整合复极 K 电流和复极储备。这会增加 HF 中的心律失常倾向,尤其是在肾上腺素应激期间。