Department of General and Visceral Surgery, University Hospital of Ulm, Albert-Einstein-Allee 23, 89073, Ulm, Germany.
Department of Internal Medicine, University Hospital of Ulm, Ulm, Germany.
BMC Med Res Methodol. 2018 Feb 13;18(1):23. doi: 10.1186/s12874-018-0476-z.
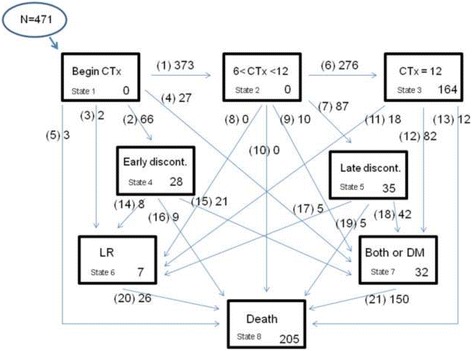
Standard survival analysis fails to give insight into what happens to a patient after a first outcome event (like first relapse of a disease). Multi-state models are a useful tool for analyzing survival data when different treatments and results (intermediate events) can occur. Aim of this study was to implement a multi-state model on data of patients with rectal cancer to illustrate the advantages of multi-state analysis in comparison to standard survival analysis.
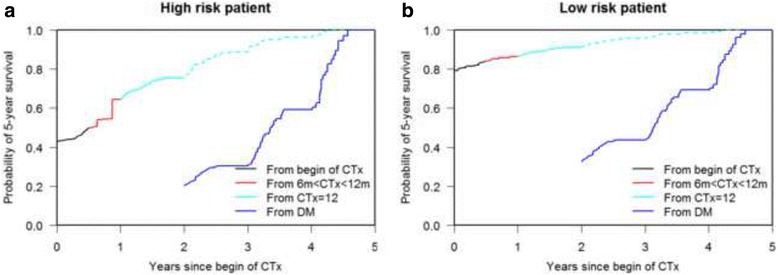
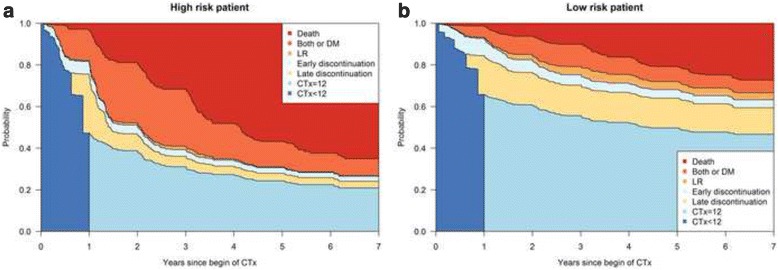
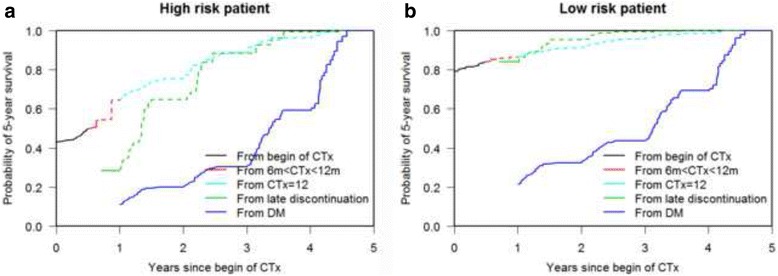
We re-analyzed data from the RCT FOGT-2 study by using a multi-state model. Based on the results we defined a high and low risk reference patient. Using dynamic prediction, we estimated how the survival probability changes as more information about the clinical history of the patient becomes available.
A patient with stage UICC IIIc (vs UICC II) has a higher risk to develop distant metastasis (DM) or both DM and local recurrence (LR) if he/she discontinues chemotherapy within 6 months or between 6 and 12 months, as well as after the completion of 12 months CTx with HR 3.55 (p = 0.026), 5.33 (p = 0.001) and 3.37 (p < 0.001), respectively. He/she also has a higher risk to die after the development of DM (HR 1.72, p = 0.023). Anterior resection vs. abdominoperineal amputation means 63% risk reduction to develop DM or both DM and LR (HR 0.37, p = 0.003) after discontinuation of chemotherapy between 6 and 12 months. After development of LR, a woman has a 4.62 times higher risk to die (p = 0.006). A high risk reference patient has an estimated 43% 5-year survival probability at start of CTx, whereas for a low risk patient this is 79%. After the development of DM 1 year later, the high risk patient has an estimated 5-year survival probability of 11% and the low risk patient one of 21%.
Multi-state models help to gain additional insight into the complex events after start of treatment. Dynamic prediction shows how survival probabilities change by progression of the clinical history.
标准生存分析无法深入了解患者在首次结局事件(如疾病首次复发)后会发生什么情况。多状态模型是分析生存数据的有用工具,因为不同的治疗方法和结果(中间事件)可能会发生。本研究的目的是在直肠癌患者的数据上实施多状态模型,以说明多状态分析相对于标准生存分析的优势。
我们重新分析了 FOGT-2 研究的 RCT 数据,使用多状态模型。基于结果,我们定义了一个高风险和低风险的参考患者。使用动态预测,我们估计随着患者临床病史信息的增加,生存概率如何变化。
与 UICC II 期相比,UICC IIIc 期的患者如果在 6 个月内或 6 至 12 个月内停止化疗,或在完成 12 个月的 CTx 后停止化疗,发生远处转移(DM)或 DM 和局部复发(LR)的风险更高,风险比(HR)分别为 3.55(p=0.026)、5.33(p=0.001)和 3.37(p<0.001)。他/她在发生 DM 后死亡的风险也更高(HR 1.72,p=0.023)。与腹会阴联合切除术相比,前切除术意味着在 6 至 12 个月内停止化疗后发生 DM 或 DM 和 LR 的风险降低 63%(HR 0.37,p=0.003)。发生 LR 后,女性死亡的风险高 4.62 倍(p=0.006)。高风险参考患者在开始 CTx 时的 5 年生存率估计为 43%,而低风险患者为 79%。1 年后发生 DM 后,高风险患者的 5 年生存率估计为 11%,低风险患者为 21%。
多状态模型有助于深入了解治疗开始后的复杂事件。动态预测显示了生存概率如何随着临床病史的进展而变化。