Chronic Disease Research Group, Minneapolis Medical Research Foundation, Minneapolis, MN
Division of Nephrology, Department of Medicine, Hennepin County Medical Center and University of Minnesota, Minneapolis, MN.
J Am Heart Assoc. 2018 Feb 13;7(4):e007231. doi: 10.1161/JAHA.117.007231.
Hospitalization for cardiovascular disease (CVD) is common among patients receiving maintenance dialysis, but patterns of readmissions following cardiovascular events are underexplored.
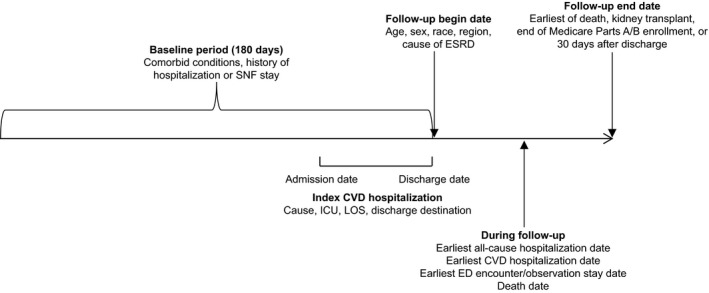
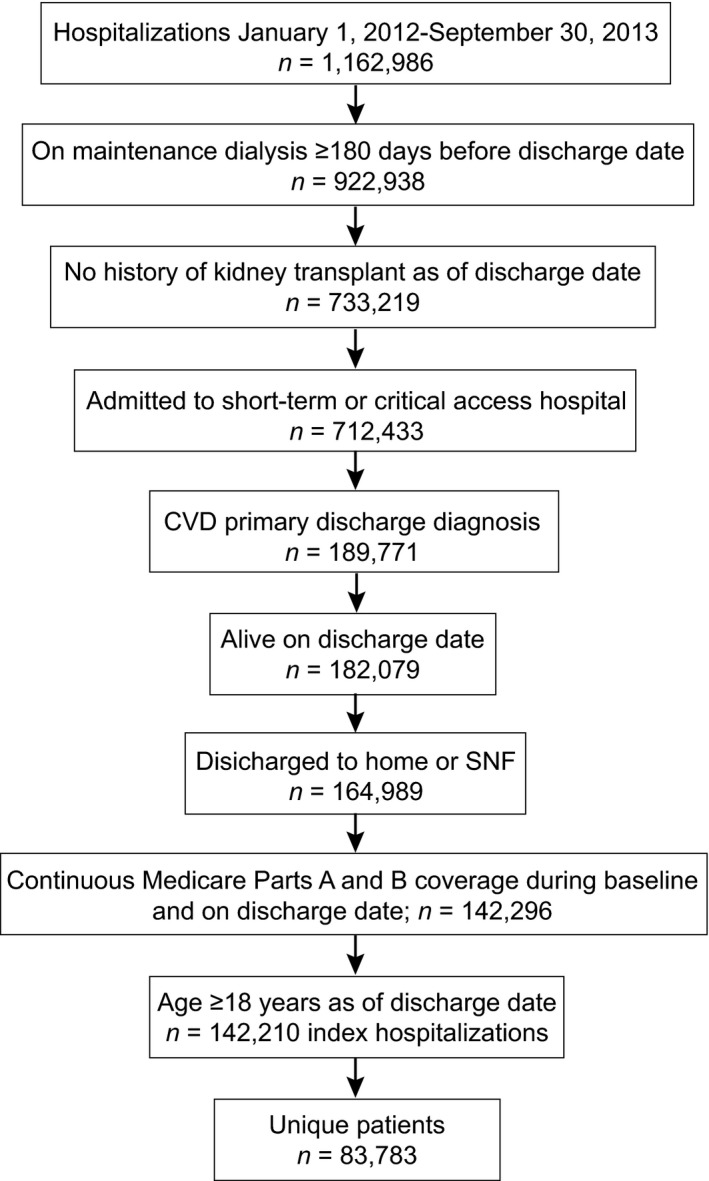
In this retrospective analysis of prevalent, Medicare-eligible patients receiving dialysis in 2012-2013, all live-discharge hospitalizations attributed to CVD were ascertained. Rates of all-cause, CVD-related, and non-CVD-related readmissions and death in the ensuing 10 and 30 days were calculated. Multinomial logistic modeling was used to assess the relationship between potential explanatory factors and outcomes of interest. Among 142 210 analyzed hospitalizations, mean age at time of index CVD hospitalization was 64.9±14.1 years; 50.4% of index hospitalizations were for women, and 41.4% were for white patients. Fully 15.6% and 34.2% of CVD hospitalizations resulted in readmission within 10 and 30 days, respectively; less than half of readmissions were CVD related (42.5%, 10 days; 43.1%, 30 days). Death within 30 days, regardless of readmission, occurred after 4.5% of index hospitalizations; 51.2% were attributed to CVD. Compared with ages 65 to 69 years, younger age tended to be associated with increased readmission risk (adjusted relative risk for ages 18-44 years: 1.55; 95% confidence interval, 1.48-1.63). Readmission risk did not differ between white and black patients, but risk of death without readmission was markedly lower for black patients (relative risk: 0.60; 95% confidence interval, 0.55-0.67).
Roughly 1 in 3 CVD hospitalizations resulted in 30-day readmission; nearly 1 in 20 was followed by death within 30 days. Risk of death without readmission was higher for white than black patients, despite no difference in risk of readmission.
心血管疾病(CVD)住院在接受维持性透析的患者中很常见,但心血管事件后的再入院模式仍未得到充分探索。
在这项对 2012-2013 年接受透析的普遍符合医疗保险条件的患者的回顾性分析中,确定了所有归因于 CVD 的全因、CVD 相关和非 CVD 相关的 10 天和 30 天再入院和死亡发生率。使用多项逻辑回归模型评估潜在解释因素与研究结果之间的关系。在分析的 142210 次住院中,指数 CVD 住院时的平均年龄为 64.9±14.1 岁;50.4%的住院患者为女性,41.4%为白人。CVD 住院的完全再入院率分别为 15.6%和 34.2%,分别在 10 天和 30 天内;不到一半的再入院与 CVD 相关(10 天为 42.5%,30 天为 43.1%)。30 天内无论是否再入院,死亡的发生率为 4.5%;51.2%归因于 CVD。与 65 至 69 岁相比,年龄较小与再入院风险增加相关(18-44 岁的校正相对风险为 1.55;95%置信区间,1.48-1.63)。白人患者与黑人患者之间的再入院风险无差异,但黑人患者无再入院死亡风险明显较低(相对风险:0.60;95%置信区间,0.55-0.67)。
大约每 3 次 CVD 住院中就有 1 次导致 30 天内再入院;近 1/20 的患者在 30 天内死亡。尽管再入院风险无差异,但白人患者的无再入院死亡风险高于黑人患者。