Perumal Nandita, Roth Daniel E, Perdrizet Johnna, Barros Aluísio J D, Santos Iná S, Matijasevich Alicia, Bassani Diego G
1Department of Epidemiology, Dalla Lana School of Public Health, University of Toronto, Toronto, ON Canada.
2Centre for Global Child Health, Child Health Evaluative Sciences, Hospital for Sick Children, 686 Bay Street, Toronto, ON M5G 0A4 Canada.
Emerg Themes Epidemiol. 2018 Feb 6;15:3. doi: 10.1186/s12982-018-0070-1. eCollection 2018.
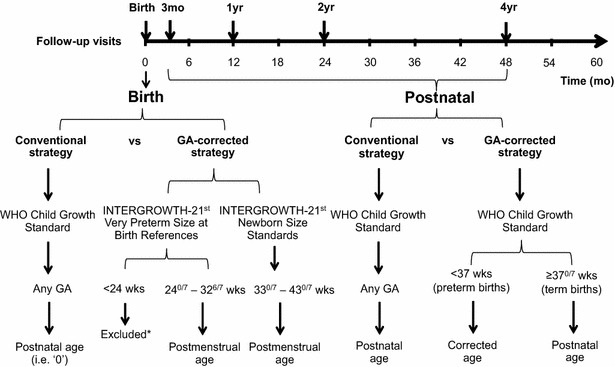
Postmenstrual and/or gestational age-corrected age (CA) is required to apply child growth standards to children born preterm (< 37 weeks gestational age). Yet, CA is rarely used in epidemiologic studies in low- and middle-income countries (LMICs), which may bias population estimates of childhood undernutrition. To evaluate the effect of accounting for GA in the application of growth standards, we used GA-specific standards at birth (INTERGROWTH-21st newborn size standards) in conjunction with CA for preterm-born children in the application of World Health Organization Child Growth Standards postnatally (referred to as 'CA' strategy) versus postnatal age for all children, to estimate mean length-for-age (LAZ) and weight-for-age (WAZ) scores at 0, 3, 12, 24, and 48-months of age in the 2004 Pelotas (Brazil) Birth Cohort.
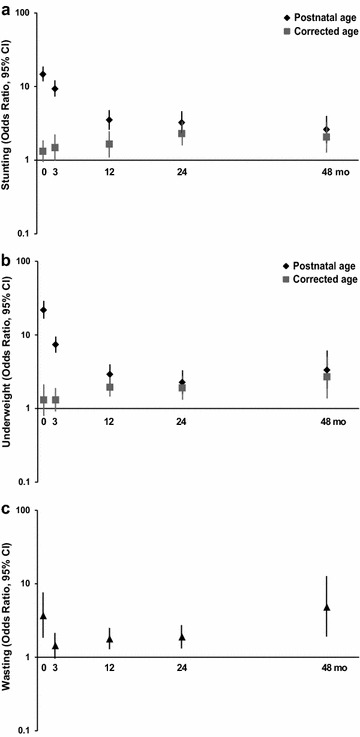
At birth (n = 4066), mean LAZ was higher and the prevalence of stunting (LAZ < -2) was lower using CA versus postnatal age (mean ± SD): - 0.36 ± 1.19 versus - 0.67 ± 1.32; and 8.3 versus 11.6%, respectively. Odds ratio (OR) and population attributable risk (PAR) of stunting due to preterm birth were attenuated and changed inferences using CA versus postnatal age at birth [OR, 95% confidence interval (CI): 1.32 (95% CI 0.95, 1.82) vs 14.7 (95% CI 11.7, 18.4); PAR 3.1 vs 42.9%]; differences in inferences persisted at 3-months. At 12, 24, and 48-months, preterm birth was associated with stunting, but ORs/PARs remained attenuated using CA compared to postnatal age. Findings were similar for weight-for-age scores.
Population-based epidemiologic studies in LMICs in which GA is unused or unavailable may overestimate the prevalence of early childhood undernutrition and inflate the fraction of undernutrition attributable to preterm birth.
在将儿童生长标准应用于早产儿(胎龄<37周)时,需要使用月经龄和/或胎龄校正年龄(CA)。然而,在低收入和中等收入国家(LMICs)的流行病学研究中,CA很少被使用,这可能会使儿童营养不良的人群估计产生偏差。为了评估在应用生长标准时考虑胎龄(GA)的影响,我们将出生时特定胎龄的标准(INTERGROWTH-21st新生儿尺寸标准)与早产儿童的CA相结合,在应用世界卫生组织儿童生长标准时(称为“CA”策略),与所有儿童的出生后年龄进行比较,以估计2004年佩洛塔斯(巴西)出生队列中0、3、12、24和48月龄儿童的年龄别身长(LAZ)和年龄别体重(WAZ)得分。
在出生时(n = 4066),使用CA时的平均LAZ较高,发育迟缓(LAZ < -2)的患病率低于使用出生后年龄时(均值±标准差):分别为-0.36±1.19和-0.67±1.32;以及8.3%和11.6%。早产导致发育迟缓的比值比(OR)和人群归因风险(PAR)在使用CA与出生时的出生后年龄时有所减弱并改变了推断[OR,95%置信区间(CI):1.32(95%CI 0.95,1.82)对14.7(95%CI 11.7,18.4);PAR 3.1%对42.9%];在3个月时推断差异仍然存在。在12、24和48个月时,早产与发育迟缓相关,但与出生后年龄相比,使用CA时ORs/PARs仍然减弱。年龄别体重得分的结果相似。
在LMICs中,未使用或无法获得GA的基于人群的流行病学研究可能会高估幼儿营养不良的患病率,并夸大早产导致的营养不良比例。