Burn Edward, Liddle Alexander D, Hamilton Thomas W, Pai Sunil, Pandit Hemant G, Murray David W, Pinedo-Villanueva Rafael
Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Botnar Research Centre, Windmill Road, Oxford, OX3 7LD, UK.
University College London Institute of Orthopaedics and Musculoskeletal Sciences, Royal National Orthopaedic Hospital, Stanmore, Middlesex, HA7 4LP, UK.
Pharmacoecon Open. 2017 Dec;1(4):241-253. doi: 10.1007/s41669-017-0017-4.
Patients with anteromedial arthritis who require a knee replacement could receive either a unicompartmental knee replacement (UKR) or a total knee replacement (TKR). This review has been undertaken to identify economic evaluations comparing UKR and TKR, evaluate the approaches that were taken in the studies, assess the quality of reporting of these evaluations, and consider what they can tell us about the relative value for money of the procedures.
A search of MEDLINE, EMBASE and the Centre for Reviews and Dissemination National Health Service Economic Evaluation Database was undertaken in January 2016 to identify relevant studies. Study characteristics were described, the quality of reporting and methods assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist, and study findings summarised.
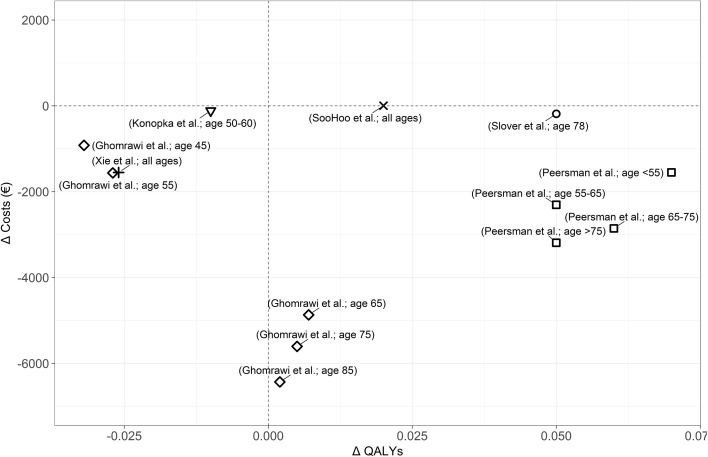
Twelve studies satisfied the inclusion criteria. Five were within-study analyses, while another was based on a literature review. The remaining six studies were model-based analyses. All studies were informed by observational data. While methodological approaches varied, studies generally had either limited follow-up, did not fully account for baseline differences in patient characteristics or relied on previous research that did not. The quality of reporting was generally adequate across studies, except for considerations of the settings to which evaluations applied and the generalisability of the results to other decision-making contexts. In the short-term, UKR was generally associated with better health outcomes and lower costs than TKR. Initial cost savings associated with UKR seem to persist over patients' lifetimes even after accounting for higher rates of revision. For older patients, initial health improvements also appear to be maintained, making UKR the dominant treatment choice. However, for younger patients findings for health outcomes and overall cost effectiveness are mixed, with the difference in health outcomes depending on the lifetime risk of revision and patient outcomes following revision.
UKR appears to be less costly than TKR. For older patients, UKR is also expected to lead to better health outcomes, making it the dominant choice; however, for younger patients health outcomes are more uncertain. Future research should better account for baseline differences in patient characteristics and consider how the relative value of UKR and TKR varies depending on patient and surgical factors.
需要进行膝关节置换的前内侧关节炎患者可接受单髁膝关节置换术(UKR)或全膝关节置换术(TKR)。本次综述旨在确定比较UKR和TKR的经济学评价,评估研究中采用的方法,评估这些评价的报告质量,并考虑它们能告诉我们这两种手术相对性价比的哪些信息。
2016年1月检索了MEDLINE、EMBASE以及循证医学与传播中心的英国国家医疗服务体系经济评价数据库,以识别相关研究。描述了研究特征,使用《卫生经济评价报告标准合并清单》(CHEERS)评估报告质量和方法,并总结了研究结果。
12项研究符合纳入标准。5项为研究内分析,另一项基于文献综述。其余6项研究为基于模型的分析。所有研究均以观察性数据为依据。虽然方法学方法各不相同,但研究通常随访有限,未充分考虑患者特征的基线差异,或依赖于未考虑这些差异的先前研究。除了评价所适用的环境以及结果对其他决策背景的可推广性外,各研究的报告质量总体上是足够的。在短期内,UKR通常比TKR具有更好的健康结局和更低的成本。即使考虑到更高的翻修率,与UKR相关的初始成本节约似乎在患者的一生中都持续存在。对于老年患者,初始健康改善似乎也能维持,使UKR成为主要的治疗选择。然而,对于年轻患者,健康结局和总体成本效益的结果不一,健康结局的差异取决于翻修的终身风险和翻修后的患者结局。
UKR似乎比TKR成本更低。对于老年患者,UKR预计也会带来更好的健康结局,使其成为主要选择;然而,对于年轻患者,健康结局更不确定。未来的研究应更好地考虑患者特征的基线差异,并考虑UKR和TKR的相对价值如何因患者和手术因素而变化。